
The obesity is a chronic disease in which environmental factors can be involved in the etiology. The aim of this study was to identify risk factors for obesity in children at Viçosa county, Minas Gerais, Brazil. Case-control study with 50 eutrophic and 50 obese children, paired according to gender, age and socioeconomic condition. This sample was selected based on nutritional evaluation of 2,074 children aged 6 to 8 years who were attending either private and public urban schools in Viçosa. Children’s and parents’ nutritional states were classified according to CDC (2000) and WHO (1998), respectively. Based on questionnaire application, the following data were collected: family structure, socioeconomic level, obesity presence and dyslipidemia in close family relatives, breast feeding, birth weight, child’s gestation conditions, feeding habits and the lifestyles of both children and parents. According to the multiple logistic regression analysis, the risk factors to childhood obesity were: the mother’s overweight (BMI ≥ 25 Kg/m2; OR: 70.49; IC: 2.17 – 182.74), the parents’ constant limitation on the foods consumed by the child (OR: 62.91; IC: 5.37 – 92.08) and frequent snack the child uses to consume in commercial establishments (OR: 10.44; IC: 1.30 – 83.92), which are mostly represented by highly energetic foods, such as fried salty foods and soft drinks (78.6%). The success of the childhood obesity treatment in this population includes the parents’ decreased overweight, mainly the mother’s, and their consciousness of the adequate feeding habit, because family’s undesirable practices contribute to the permanence of obesity in childhood, such as constant limitation of ingested foods and frequent snacks in commercial establishments.
Key words: Child, parents, risk factors, obesity, case-control studies.
La obesidad es una enfermedad crónica en la que factores ambientales pueden estar relacionados en su etiología. El objetivo de este estudio fue identificar factores de riesgo para la obesidad en niños del municipio de Viçosa, Minas Gerais, Brasil. Se trata de un estudio del tipo caso-controle, con 50 niños eutróficos y 50 obesos, pareadas de acuerdo con el sexo, la edad y la condición socioeconómica. La muestra fue seleccionada a partir de la evaluación nutricional de 2074 niños en la franja etaria de 6 a 8 años matriculados en escuelas públicas y privadas en Viçosa. El estado nutricional de los padres de estos niños fue clasificado de acuerdo con el CDC (2000) y WHO (1998), respectivamente. Por aplicación de un cuestionario, fueron colectados datos sobre estructura familiar, nivel socioeconómico, presencia de obesidad y dislipedemas en familiares próximos, amamantamiento materno, peso de nacimiento, condiciones de gestación del niño, hábitos alimentares y estilos de vida del niño y de los padres. De acuerdo con el análisis de regresión logística múltipla, los factores de riesgo para la obesidad en la niñez fueron: el exceso de peso materno (IMC > 25 kg/m2; OR: 70.49; IC: 2.17 – 182.74), límite constante puesto por los padres de alimentos consumidos por el niño (OR: 62.91; IC: 5.37 – 92.08) y merienda frecuente en establecimientos comerciales por los niños (OR: 10.44; IC: 1.30 – 83.92), siendo este representado en su mayoría por alimentos de alto contenido energético, tales como meriendas fritas y refrescos (78.6%). El éxito del tratamiento de la obesidad infantil en esta población incluye la disminución del sobrepeso en los padres, principalmente de la madre, la concienciación de éstos en relación a los hábitos alimentarios, toda vez que prácticas familiares inadecuadas tales como meriendas frecuentes en establecimientos comerciales, contribuyen a la permanencia de la obesidad en la niñez.
Palabras clave: Niño, padres, factores de riesgo, obesidad, estudios de casos y controles.
Nutrition and Health Department, Federal University of Viçosa, Minas Gerais, Brazil
Study financed by FAPEMIG (Research Supporting Foundation of Minas Gerais State).
Obesity is considered as an emerging public health problem in Brazil and throughout the world. It constitutes one of the main nutritional offences in children, and can lead to negative consequences for the physical and mental health. Besides, it is considered as an obesity predictor in adult life, as being able to cause a risk situation, which might lead to increased mortality as a cause associated to atherosclerotic disease, to hypertension and to metabolic alterations.
Because difficulty to obtaining a successful obesity treatment in the adult life, it is necessary to develop prevention programs as soon as at childhood. Golan et al. (1) observed the treatment of the children’s obesity to be more effective when working with their parents, since they are considered as the main changing agents. In children, the reduction in both fat and sugar intake may be obtained by changing the parents’ feeding habits, which might extend to all other family’s members (2).
It is worth to emphasize that obesity is not synonymous of health, because despite the excessive food intake and the consequent high caloric consumption, usually there are deficits of those nutrients necessary to the growth and adequate organism development, mainly in the childhood, when those processes are intensive. The better way to solve this problem seems to be the balanced feeding based on the family’s feeding reeducation and mainly the child’ (3).
Identifying the factors that influence the development of obesity in childhood is important, in the sense to establishing positive modifications in the child’s lifestyle (4). Investigative studies of the risk factors for obesity in the childhood in populations, as taking into account the geographical and cultural aspects, are necessary for assigning effective efforts to local prevention. In Brazil and developing countries, few casecontrol studies have been developed to investigate the risk factors for obesity in children. In this context, a study was carried out to evaluate the risk factors for obesity in children, in Viçosa county, Minas Gerais, Brazil, as well as to contribute for the directness of effective orientation conducts, aiming at either the prevention of obesity in childhood and subsequent stages of the life and the reduction of this nutritional disturbance and associated chronic diseases, that are increasing in the modern world.
This was a case-control survey carried out in the urban area of the city of Viçosa, addressing only children.
The study was carried out in all public and private (18 and 7, respectively) urban schools in Viçosa, Minas Gerais, Brazil, that assisted the children at the age range from 6 to 8 years and spontaneously accepted to participate into this study. Only a public school did not participate in this study, because nonauthorization by the respective school direction. All scholars aged 6 to 8 years (n = 2,074) enrolled in the respective schools were weighed and measured. From the weight and height measures checked in appropriate places in the respective schools, the body mass index (BMI) was calculated and based on age and gender, the children’s nutritional state were defined according to the anthropometric reference preconized by the Center for Disease Control and Prevention (CDC) (5). The cutting points used for classification of the overweight and obesity were based on classification proposed by Must et al. (6): overweight (≥ percentile 85 and < percentile 95) and obesity (≥ percentile 95).
Due to variation of the potential risk factors for obesity among different ages, gender, and socioeconomic conditions, this was a case-control study where the obese children were paired with the eutrophic ones at proportion 1:1, according to gender, age group, and classroom, consequently according to school and socioeconomic condition. The obese children presenting BMI/age equal or above the percentile 96 were included into sample, since the increased of cutting point specificity reduces the possibility to obtain false-positive children in the sample. The selection criterion for the eutrophic children (5 ≤ BMI/age < 85) was based on randomly choosing the children with the same gender and classroom as the obese’ as well exactly the same age, represented by a number with two decimals. By anthropometric evaluation accomplished in schools, a total of 58 (2.8%) children were found to be obese (≥ percentile 96). Because the loss of 8 obese children (6.9%), their eutrophic pairs were not appraised (eight). The sample of this study was composed by 100 children, that is 50 obese and 50 eutrophic ones. Because ethical matter, those mothers whose children showed low weight and overweight, were informed about their children’s nutritional state and were assigned to the public health service, where the individual nutritional service was accomplished.
Initially, the selection of the obese and eutrophic children’s groups were established from BMI/age. After definition of both groups, the parents were invited by telephone to participate in the study, and a schedule was established for a personal encounter over which all participants gave written consent. The data collection was accomplished in the Nutritional Evaluation Laboratory pertaining to the Department of Nutrition and Health of Federal University of Viçosa. This study was approved by the Ethics Committee of Federal Univesity of Viçosa.
All anthropometric evaluation was only accomplished by one author of this study in order to avoid possible biases in verifying the measures. In the evaluation of children’s and parent’s nutritional state, the weight was obtained by a portable, digital and electronic scale with 150kg capacity and 50g division. Height was verified with 2m-extension stadiometer, that was divided into centimeters and subdivided into millimeters. The techniques proposed by Jelliffe (7) were applied to verify both measures. The parents’ nutritional state was classified according to World Health Organization (WHO) (8): low weight (BMI < 18.5), eutrophy (18.5 ≤ BMI < 25.0), overweight (25.0 ≤ BMI < 30.0) and obesity (BMI ≥ 30.0).
The questionnaires were applied to the mothers, but to the child’s responsible in the case this was impossible. They were elaborated by the authors and were tested previously with 30 mothers of children of same age group to the one of the study, not included in the sample of this work. These questionnaires included the family aspects, the conditions of gestation and child’s birth, breast-feeding time, feeding habits and the physical activity practices accomplished by children and their parents, as well as the presence of obesity and dyslipidemia in close relatives. Concerning to family aspects, the following were analyzed: the home room numbers; total number of people living in the child’s home; his/her brother and sister numbers; if the parents have remunerate activities or not; education level; and the presence of tobacco and drinking habits among them. In relation to the aspects of mother’ gestation and child’ birth condition, the mothers were interrogated about maternal tobacco habit and weight gain in gestational period, as well as the child’s weight at birth, the type and duration of breast feeding. The value above 16kg for the mother’s weight gain during gestation was considered as excessive one (9). The birth weight values between < 2.500g, 2.500 |- 3.000g 3.000 |- 4.000g and ≥ 4.000g were considered low, insufficient, normal and excessive, respectively (10). When the child consumed mother’s milk only, a case of exclusive breast feeding was considered.
The mothers were questioned about their children’s actual habit to have regular meals at established schedules, if they have the habit to eat at meal intervals and/ or substitute them by snacks, as well as the number of daily meals they have during week days. They were also questioned if their children have the meals together the family, and if they have the habit to take a snack frequently in commercial establishments, as well as how much daytime they spend in front of television and their sedentary activity practices during weekdays and weekend, such as to watch television, to play videogame and to use computer.
Based on mothers’ information, the parents’ attitude were appraised in relation to their children’s feeding, such as a constant limitation of the foods they use to consume. The mothers were questioned about their own behavior relative to feeding habits and lifestyle, such as actual habit to have regular meals at established schedules, the habit to eat at meal intervals or to substituting the meals by snacks, number of daily meal they have during weekdays, daily time spent in front of television, as well as the accomplishment of physical activity at leisure time. For those items, the mothers were questioned about their children father’s behavior.
The mothers or child’s responsible person were questioned about the presence of obesity and dyslipidemia in the child’s close relatives [mother, father, grandmother and grandfather, uncles and aunts (both maternal and paternal)].
The database and the statistical analyses were accomplished in the softwares Epi Info version 6.04 (11), Sigma-Stat (12) and Statistical Program for Social Sciences (SPSS for Windows 10.0). To verify the distribution of the variable values were normal, the Kolmogorov-Smirnov normality test was used (13). The association between each factor and children’s obesity were analyzed, by applying the qui-square test for paired sample, and the odds ratio (OR) and the confident interval (CI) of 95% calculated for each factor (14). In the multiple logistic regression analysis, only the variables with p < 0.20 of the univariate analysis were included (15). To compare the averages or medians of the variables between the paired groups, the paired t-test and Wilcoxon test were respectively used (12). A probability below 5% was considered as significant statistical level.
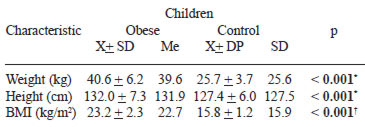
Table 1 shows the children’s values for weight, height and BMI, which were superiors in the obese ones relative to the eutrophic ones (p < 0.001). In this study, the children’s average age was 7.8 years.
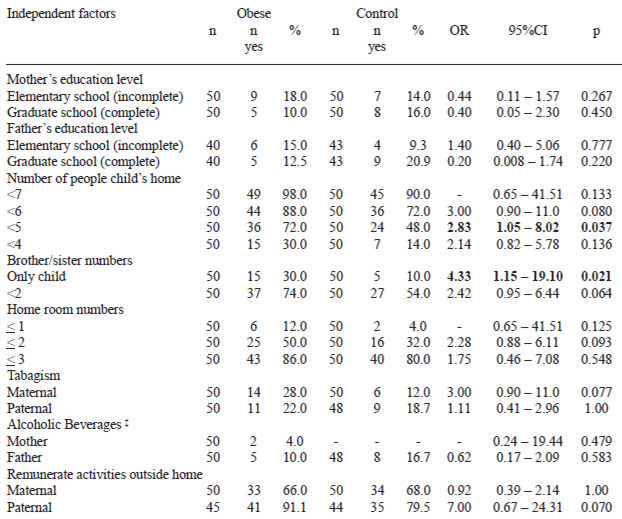
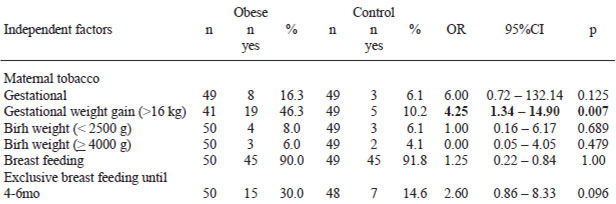
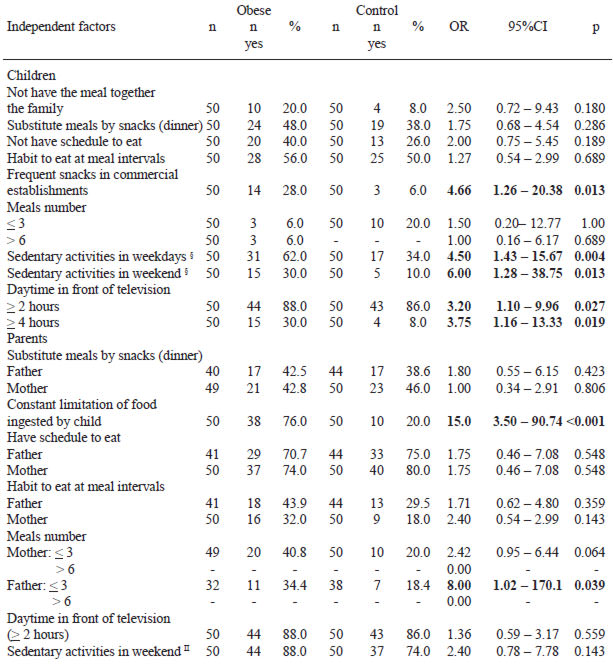
Tables 2, 3, 4 and 5 show the results obtained by the quisquare test for all categorical factors included into this study. Based on univariate analysis, it is observed that several variables showed to be associated to childhood obesity (Tables 2, 3, 4 and 5). Despite of this high number of potential factors included into investigation as well as the variables associated to obesity, only three variables were identified as risk factors for the multiple logistic regression analysis. The mother’s overweight (BMI ≥ 25 kg/m2), the children’s frequent snack in commercial establishments, and the parents’ constant limitation upon the foods consumed by their children were considered as risk factors associated to children’s obesity in Viçosa county in the final logistic regression (Table 6). It is worth to emphasize that most snack types (78.6%) accomplished in commercial establishments mentioned by obese children’s mothers were based on soft drinks and “junk food” (chips, doritos, tortilhas, french fries – data not given in table).

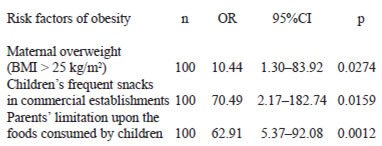
Despite of the high number of factors included into investigation, a few risk factors were associated to childhood obesity. The following risk factors were identified for obesity in scholars at the urban area of Viçosa county: mother’s overweight (BMI ≥ 25 kg/m2); frequent snack consumption by the child in commercial establishments; and the parents’ constant restriction on the amount of foods the children use to consume.
The mother’s obesity shows to be a risk factor for obesity at childhood in several available studies (16-19). It is well known that parents’ obesity is strong predictor for children’s excessive weight, as a possible result from either genetic and environmental influences, mainly in the family example given for feeding habits and undesirable lifestyles developed inside the own home.
In this study, no association were found between the father’s overweight and children’s obesity. Perhaps, the higher maternal influence on the children’s nutritional state, compared to the paternal’, might be justified the mother’s proximity with her child’s education and by direct care, therefore interfering into feeding and lifestyle adopted by her child, who tends to be similar to the mother’. According to Marins et al. (19), the influence of the parents’ nutritional state on their children’s obesity, partly due to genetic components, is also strongly determined by the family’s food intake. According to the authors, it is important to emphasize that usually the mother’ feeding habit tends to be adopted by the family and by the child, because mothers are more involved into preparation and choice of the foods in home. Similar results were observed by Oliveria et al. (20) and Nguyen et al. (21), who verified the children’s feeding to be more similar to the mother’ than to the respective fathers’. Hui et al. (18) verified that both parents’ overweight (BMI ≥ 25 kg/m2) were significantly associated to overweight in 6 and 7 years-old children, and it should be emphasized that the association strength between mother’s obesity and child’s overweight was almost double the father’s obesity. When analyzing the combined influence of the anthropometric and socioeconomic variables on the childhood obesity, Kain et al. (16) observed that mother’s obesity was the factor most correlated with this nutritional disturbance. According to the authors, this fact implicates the prevention actions against childhood obesity must involve the mother in order she also adopts healthy life habits, therefore being able to transmit them to their children.
In the present study, the children’s frequent habit to take a snack in commercial establishments was a risk factor associated to obesity, because the main ingested foods (mentioned by mothers) showed high energy contents, which could favor the excessive body weight when consumed frequently. The inadequate feeding habit represented by frequent consumption of highly energetic foods is already shown as clearly associated to the childhood overweight (22,23). In the prevention of obesity, the emphasis on consumption of fruits and vegetables could represent an important step to avoid preparations with high energy density (24). It is well-known that genetic factor can predispose the individual to obesity. However, the family posture in particular the feeding practices and other behavioral variables, such as diet composition and the physical activity patterns serve as a catalyst for the expression of obesity (25).
In this study, the parents’ constant limitation on the foods consumed by their children was also a risk factor for childhood obesity, since the forbidden foods rather become the favorite ones by the children. When they have access to those foods, these ones are usually consumed at high amounts, therefore causing reactions contrary to the parents’ objectives, besides the possible loss of the satiation capacity caused by such an excessive control upon children’s feeding.
In childhood, many parents stimulate their children to eat certain foods, and according to Birch et al. (26) they consume them at lower amounts. Those forbidden foods can be excessively consumed when the child has access to them (27). Those children whose mothers control their feeding intake become less able to regulate the own feeding intake (25).
The parents have strong influence upon the intake of foods by their children. However, the more the parents insist on the consumption of certain foods the smaller is the probability their children will consume them. In the same way, the restriction by the parents might have deleterious effects. According to Spruijt-Metz et al. (28), the restrictive feeding practices due to the concern with the child’s weight are associated to highly energetic intake and high BMI values, whereas the parents’ pressure for the child to eat because thinking the child is thin is associated to low energy intake and low BMI. Those children whose parents had higher feeding restrictions showed higher body fat increase than those whose parents had lower restrictions. As the prejudicial effects from the dietary restriction on obese children in the long run are known, valuable alternatives such as changes in the lifestyle and interventions increasing the body image and self-esteem are recommended (29). In childhood, the parents are advised to supply to their children with healthy and balanced meals and snacks, with appropriate nutrients that would allow the children to choose both quality and amount of those healthy foods they want to eat (30). According to Bellisle (31), the children’s hunger and satiation sensations are always unknown by the adults, who try to instruct them to feeding according to the rules accepted by society, as well as according to the family’s own habits. Difficulty in establishing a good satiation control is a risk factor for the development of obesity either in childhood and adult life.
Studies have been carried out to investigate the risk factors for obesity in the childhood (17,18,32). It is particularly difficult to compare those results with ours’, since they proceed from different population studies as each one with its own geographical, cultural and behavioral determinant, besides the different definition for obesity. However, some similar results have been found, such as for mother’s obesity. Hui et al. (18) observed that the parents’ obesity, high birth weight, short sleep time, high energy intake, as well as to have father actually smoker were risk factors for obesity in 6- and 7-years old children in Hong Kong/China. He et al. (17) studied children from 1mos- to 6.9 years-old in 8 Chinese cities, and verified the family’s history for obesity, high birth weight, and fast eating habit were risk factors for obesity in those children. However, Locard et al. (32) found the short sleep duration to be the most important risk factor for obesity in 5-years old children living in France. Differences in the methodologies for classification of obesity, as well as differences in the populations’ cultural and social patterns probably contribute for the inconsistent discoveries.
One of the limitations of the present work is the fact that is was a retrospective study in which memory and answering biases by the mother may have interfered. Poor ability to remember some questions of the questionnaire can be occurred, for instance, for the duration of breastfeeding, birth weight, gestational weight gain, number of obese close relatives and number of close relatives with dyslipidemia.
In spite of this study to emphasize the investigation of risk factors associated to childhood obesity, its interpretation should be cautiously performed, since this work showed a transverse design, therefore the causal denotation should be carefully interpreted. In addition, it is important to emphasize the size of the sample as a limiting factor in this study, that occurred due to the lowest obesity prevalence found in Viçosa county - Brazil, since methodological care was taken to use the cutting point for obesity (BMI/age ≥ percentile 96) that was superior to the one preconized (BMI/age ≥ percentile 95), with the objective to eliminate the positive-false ones, exactly for is being a transverse-type study. So, the obesity prevalence in Viçosa (2.8%) was lower than that found in other studies carried out in Brazil and developed countries with children at the same age range (33-37). However, it is important to highlight that 100% infantile population at the age range from 6 to 8 years enrolled in Viçosa’s private and public urban schools, who accepted to participate in this study, were evaluated with the methodological care concerning to increased of cutting point specificity for obesity in order to reduce the falsepositive ones, with basically 100% obese children (BMI/age ≥ percentile 96) included into investigation. It was decided to study the total population instead of an estimated sample in order to provide higher consistence to the statistical analysis, therefore a better reliability on the results.
The elucidated risk factors associated to obesity in children at Viçosa county’s urban area, Brazil, can be useful to the directness of effective orientation conducts, targeted to the prevention of obesity in childhood and subsequent stages of life, as well as the reduction of this nutritional disturbance and the associated chronic diseases, both rising in the modern world. The success of the obesity treatment in childhood includes own monitoring, change in the feeding behavior, and the parents’ reduced overweight (mainly the mother’s), which will probably contribute to positive modification of child’s feeding and lifestyle. Besides, the parents’ conscientiousness is extremely important in the search for elimination of the undesirable family practices that contribute to the permanence of obesity in childhood, such as the constant limitation of the ingested foods and accomplishment of frequent snacks in commercial establishments.
The authors thank to Improvement Coordination of Graduate-Level Staff (CAPES) by the scholarship, to Research Supporting Foundation of Minas Gerais State (FAPEMIG) by financing the project, to the Health and Nutrition Department of Federal University of Viçosa by the support, to the children and their parents by their participation in this study.
Recibido: 28-01-2008
Aceptado: 25-08-2008