
Metabolic Syndrome is a complex clinical condition that brings together a set of cardiovascular risk factors. Lifestyle changes, such as eating habit improvements, are first-choice therapies for the treatment of this clinical condition. This study aimed to evaluate the effect of short-term nutritional counseling, on the diet quality and total energetic value (TEV) in individuals with Metabolic Syndrome. Eighty subjects (men and women) aged 30 to 60 years with metabolic syndrome were followed over three months. The Healthy Eating Index tool adapted to the Brazilian population was used for the evaluation of diet quality. Mean age was 51 + 6 years, and 68.6% were women. The mean score of the dietary quality of the population studied increased significantly from 53.02 to 61.65 after intervention. The amount of individuals classified as Inappropriate Diet decreased significantly six-fold, the amount of individuals classified as Healthy Diet increased four-fold, and the percent of diets classified as Diet that Needs Change decreased by 25% when compared to the beginning of the study. Adequate intake of vegetables was inversely associated to abdominal circumference, as well as adequate intake of sodium and fasting serum insulin. The amount of TEV presented a significant reduction (p <0.000) after intervention. The short-term nutritional counseling showed to be efficient to improve dietary quality. Associations between dietary quality and variables studied highlight the importance of nutritional intervention in individuals with metabolic syndrome.
Key words: Metabolic Syndrome X, nutrition therapy, risk factors, motor activity, omega-3 fatty acids
A Síndrome Metabólica é uma condição clínica complexa que reúne um conjunto de fatores que aumentam o risco cardiovascular. Mudanças no estilo de vida como a melhora dos hábitos alimentares são consideradas terapia de primeira escolha nesta condição clínica. Este estudo tem como objetivo avaliar o efeito de uma intervenção nutricional de curta duração sobre a qualidade da dieta e o valor energético total (VET) em indivíduos com Síndrome Metabólica. Oitenta indivíduos (homens e mulheres) com idades entre 30 a 60 anos, com síndrome metabólica foram acompanhados ao longo de três meses. Para avaliar a qualidade da dieta foi utilizado o instrumento Índice de Alimentação Saudável adaptado para a população brasileira. A média de idade foi de 51 + 6 anos e 68,6% eram mulheres. A pontuação média da qualidade da dieta da população estudada aumentou significativamente de 53,02 para 61,65 após a intervenção. A quantidade de indivíduos classificados como dieta inadequada diminuiu significativamente em seis vezes, a quantidade de indivíduos classificados como dieta saudável aumentou quatro vezes, e a percentagem de dietas classificadas como dieta que necessita modificação diminuiu 25% em relação ao início do estudo. A ingestão adequada de vegetais foi inversamente associada à circunferência abdominal, bem como a ingestão adequada de sódio e insulina sérica de jejum. O VET apresentou uma redução significativa (p <0,000) após a intervenção. O aconselhamento nutricional de curta duração mostrou-se eficiente para melhorar a qualidade da dieta. As associações entre a qualidade da dieta e as variáveis estudadas destacam a importância da intervenção nutricional em indivíduos com síndrome metabólica.
Palavras chave: Síndrome X Metabólica, terapia nutricional, fatores de risco, atividade motora, ácidos graxos omega- 3
Pontifical Catholic University of Rio Grande do Sul (PUCRS). Porto Alegre - RS - Brazil. University of Santa Cruz do Sul (UNISC). Cruz do Sul – RS – Brazil.
The Metabolic Syndrome (MS) is a complex disorder represented by a set of cardiovascular risk factors usually related to the central storage of fat and to insulin resistance (1). From an epidemiologic standpoint, this syndrome is responsible for an increase of around 1.5 times in general mortality and of 2.5 times in mortality due to cardiovascular reasons (2).
According to the World Health Organization (WHO), four of the six most important morbid-mortality risk factors associated to chronic diseases (systemic arterial hypertension, hypercholesterolemia, insufficient intake of fruits, vegetables, overweight and obesity, physical inactivity, smoking) are related to diet (3).
Interventions that give priority to the improvement of diet quality affect several criteria of the MS, thus reducing the risk of cardiometabolic complications (4,5).
Nutritional counseling for a healthy diet should be the first management approach adopted in the treatment of MS, aiming to reach or maintain the weight considered adequate, to decrease levels of total cholesterol, LDL, TG, as well as to increase HDL levels (6). Nutrition directly effects lipidic profile and body weight. An efficient intervention is based on the development of an individualized nutritional plan capable of preventing a sustainable decrease in weight between 5 and 10% of the initial body weight (4).
The evaluation of food intake plays an important role in providing subsidies for a nutritional intervention focused on the improvement of eating habits. Specific needs or characteristics of a diet, which may predispose or worsen diseases, need to be addressed in food intake evaluations. An analysis tool that identifies inadequate eating habits provides data for an intervention directed towards the need for change (7).
Dietary evaluation tools, such as the Healthy Eating Index (HEI), were developed by the United State Department of Agriculture’s (USDA) Center for Nutrition Policy and Promotion (CNNP), based on the work of Kennedy et al, to measure how well diets adhere to the recommendations of the Dietary Guidelines and to assess diet quality using a single composite number (7).
The HEI proposed in 1995 was considered by the American Dietetic Association as an adequate tool to measure diet quality in the American population and to create a gradient that reflects risk for many chronic diseases related to nutrition (8). Its design was based on the importance of certain nutrients and on dietary recommendations of the Food and Nutrition Board (9).
In 2004, Fisberg et al. (10) adapted the HEI for the Brazilian population (10). Since then, this tool has been increasingly used, at first the HEI adapted for Brazilians (HEI BR) was used with adolescents. However, in Brazil and in the world this tool is rarely used in the population with MS and other non-transmittable chronic diseases.
Considering the relevance of treatment with nutritional counseling for a healthy diet, the present study aimed at evaluating the effect of a short-term nutritional counseling for a healthy diet, on the dietary quality and total energetic value in individuals with MS.
The sample totaled 80 individuals (men and women aged 30 to 60 years), and sixty-seven completed the follow-up over three months. The sample consisted of secondary data basis from a major study. The metabolic syndrome was defined according to criteria by the Third Report of the U.S. National Cholesterol Education Program Adult Treatment Panel (NCEP ATP III), that is, abdominal circumference >88 cm for women and >102 cm for men; systolic blood pressure >130 mmHg and diastolic blood pressure >85 mmHg; fasting glucose >100 mg/dl; triglycerides >150 mg/dl; cholesterol HDL <40 mg/dl for men and <50 mg/dl for women (4). Data collection was conducted from August 2006 and June 2008. The sample was screened via ads published on communication medias (newspapers, radios, neighborhood newsletters).
The following exclusion criteria were considered: use of medications for weight reduction and/or lipidlowering drugs, history of cardiovascular event, body mass index >40 kg/m² (BMI calculated as kg/height²) (11), pregnancy, use of an antidepressant medication, hypothyroidism; out of reach and/or did not show for follow-up.
The research protocol was started after approval by the Ethics in Research Committee of Pontifical Catholic University of Rio Grande do Sul (PUCRS) and written informed consent was obtained from all the volunteers.
Anthropometry and body composition assessments: Body weight was obtained to the nearest 00.1 kg with a mechanical balance Cauduro®, with a capacity of 160 kg, using the minimum possible clothing and no shoes. Height was measured without shoes while standing on a level, hard surface using a stadiometer, with 2 m of height and accurate to 0.5 cm. Waist circumference was measured at the maximum extension of the abdomen as recommended by Lohman et al (12), using an common inextensible and inelastic tape measure with 150 cm in length.
Nutritional counseling: Nutritional intervention was performed by trained professionals. The monitoring occurred individually and lasted three months. The initial and final assessment comprised the food records, measurement of weight, height and waist circumference. Dietary intake was measured by the 24-hour recall method and two food records (one week day and one we ekend day) before and after the intervention. After the evaluation, individualized dietary plans were delivered to each patient.
The food plan was based on recommendation of the NCEP ATP III (4), which encourages the following composition: Total calories: to reduce weight in 5% to 10%; carbohydrates: 50-60% of total calories, with emphasis on complex carbohydrates; fibers: 20-30g/day; total fat: 25%-35% of total calories; saturated fatty acids: < 10% of total calories; polyunsaturated fatty acids: up to 10% of total calories; monounsaturated fatty acids: up to 20% of total calories; cholesterol: <300 mg/day; protein: 0.8 g to 1.0 g/kg present weight/day or 15% of total calories; micronutrients: as recommended by DRIs (13).
The follow-up visits occurred every two weeks, totaling six consultations, to discuss changes in eating habits, nutrition guidelines, and the importance of compliance with the diet to promote weight loss and to improve the quality of health. The dietary intervention included written and oral instructions in the form of lecture, with the aid of a sequence of posters. The achievement of goals and main difficulties to adhere to diet were verified in all consultations, and topics on healthy eating: labeling of foods, trans fats, functional foods, food pyramid, sodium intake, encouraging to eat at least five portions of a variety of fruit and vegetables a day, and clarification of doubts were approached.
The recommended dietary plan was organized from calorie equivalents. The food groups and servings sizes of each food group were established in accordance with the Brazilian Adapted Food Pyramid (14). Four groups of calorie levels were established, in accordance with the recommendation of 20 to 25 kcal/kg (15), aiming at the weight loss of 5% of initial weight within 3 months (4). The four groups of calorie levels established were: 1,600, 1,900, 2,200 and 2,500 kcal per day. Homemade measures of food records were converted into grams and milliliters and the quantification of nutrients was done using the computerized program of the São Paulo School of Medicine Nutwin®. Reference measurements as per the size of servings were based on Brazilian Adapted Food Pyramid (14). In this program the data of the Brazilian Table of Food Chemical Composition (TACO in its Portuguese acronym) was included (16).
The HEI Adapted to Brazilians: The HEI Adapted to Brazilians (HEI BR) is the sum of 10 component scores. Components 1 to 5 measure the degree to which a person’s diet complies with the Brazilian Adapted Food Pyramid recommendations for the 5 major food groups: Grains (bread, cereal, rice, and pasta), Vegetables, Fruits, Dairy (milk, yogurt, and cheese), and Meat, eggs and beans (meat, poultry, fish, dried, eggs, beans and nuts). Components 6 to 9 assess compliance with recommendations for total fat, saturated fat, cholesterol, and sodium intakes. The intakes of saturated fat, total fat, cholesterol, and sodium were scored with 10 points if saturated fat ≤10% of energy, total fat ≤30% of energy, cholesterol <300 mg, and sodium < 2400 mg. A zero score was given for >15% of energy for saturated fat, > 45% of energy for total fat, cholesterol >450 mg, and sodium >4800 mg. Between these 2 cutoffs, scores were scaled proportionately. The final component examines the variety of foods in the diet (similar foods, such as oranges and orange juice, are considered one item toward variety). A total intake of food from fifteen different food groups or more per day was assigned a score 10, while the food intake from five different food groups was assigned a score 0. Intermediate amounts were assigned scores according to their amounts. Each component is scored from 0 (for lack of compliance) to 10 (for full compliance), with intermediate scores calculated to indicate degree of compliance with dietary recommendations. The total HEI BR score ranges from 0 (worst) to 100 (best) (10).
The HEI BR was calculated before and after the intervention, using the three food records, including 1 weekend day, provided by each patient. The HEI BR value of each volunteer represents the mean of these three records.
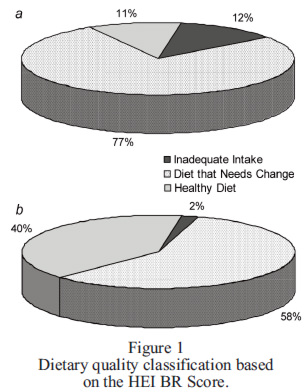
The final score of each evaluated component was totaled up, resulting in a final score which classifies the diet quality as: Inadequate Diet = below or equal to 41 points; Diet that Needs Change = higher than 41 and lower than 64 points; Healthy Diet = equal to or higher than 64 points (10).
Biochemical measurements: Blood samples were collected after a 12-h overnight fasting by venous puncture. Plasma glucose, serum total cholesterol, serum triglyceride and serum HDL-cholesterol concentrations were measured by standard enzymatic methods using reagents in a fully automated analyzer (Vitros 950 dry chemistry system; Johnson & Johnson, Rochester, NY). LDL-cholesterol was estimated using the Friedewald equation (17).
Statistical Methods: Data was summarized and classified according to frequency and percentage (for the category variables), and mean and standard deviation (for continuous variables). Student's t-test was used to measure the effect of changes before and after intervention on HEI BR components. For associations between HEI BR, total energetic value (TEV), anthropometric profile, serum and arterial blood pressure variables, Pearson's linear correlation coefficient and multiple linear regression were used. The significance level was p < 0.05.
.The results refer to a total of 67 participants who completed the 3-month monitoring period. Thirteen volunteers were excluded from the study because they could not attend more than two consecutive appointments.
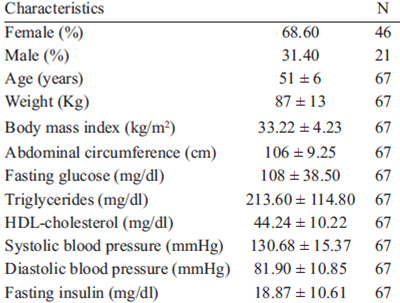
Mean age of the population studied was 51 + 6 years, and 68.6% were women. The study population characteristics are described in Table 1.
In the beginning of the study, during HEI BR analysis, volunteers presented low scores (<4) for the components: Vegetables, Fruit and Sodium, which demonstrate low intake adequacy of these nutrition groups. Intermediate scores (≥4 and <6,4) where observed for the following components: Grains; Dairy; Meet eggs and beans; Total fat and Variety; and high scores (>6,4) were recorded for Cholesterol and Saturated Fat. At the end of the follow-up none of the assessed diet components presented a low mean score. Score amounts that were low in the beginning of the intervention changed to intermediate. Intermediate and high scores stayed within this point cut after intervention.
The highest percentage noticed for the zero score before and after the intervention, which indicates in adequate intake, was found for the component Fruit. On the other hand, the highest percentage for the 10 score was associated to Cholesterol, during both steps of the study.
The effects of the short-term nutritional counseling program over the dietary quality and total energetic value of the volunteers who participated on the study are described in Table 2.
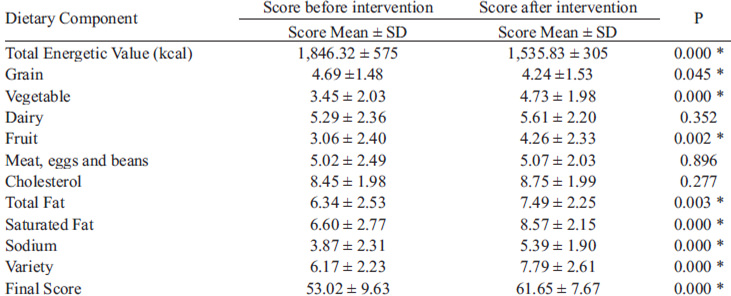
Nutritional counseling significantly improved the HEI BR's Final Score. The study population presented a significant reduction in values of TEV, an improvement in the Total Fat, Saturated Fat, Sodium and diet Variety scores.
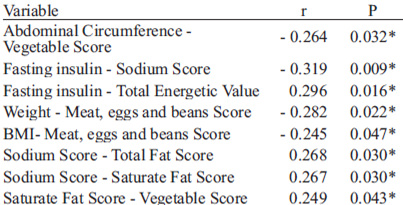
A significant improvement in the intake adequacy of the Fruit and Vegetables scores was also observed (Table 3). The linear correlation coefficient analysis demonstrated a statistically inverse association (p<0.05) between an adequate vegetable intake and abdominal circumference, indicating that the more the diet in the Vegetables group approached the recommended values, the smaller was the abdominal circumference we observed. A high score of the Sodium component was associated to smaller levels of serum insulin. Thus, the Sodium component also had a positive association with the Total Fat and Saturated Fat components, which suggests that, in this population, the smaller the amount of sodium intake, the lower total fat and saturated fat intake was observed in the daily diet. There was a positive association between daily values of energy intake and fasting serum insulin. The values of energy intake were inversely associated with adequate cholesterol intake, that is, in this population, the higher the total energy values, the smaller the score for Cholesterol component intake.
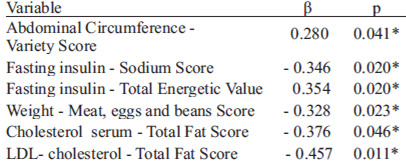
The multiple linear regression models showed a positive association between abdominal circumference and Variety component. A positive association has also been found between serum insulin and TEV. In contrast, a negative association was noticed between serum insulin and the Sodium score variation in HEI Adapted. There was a negative association between the Meat, eggs and beans group variation and body weight. Finally, HEI BR Total Fat component had a negative association with the variance of total cholesterol serum and serum LDL cholesterol (Table 4).
Before the intervention, 12.12% of the volunteers presented Inadequate Diet, 77.28% presented Diet that Needs Change, and 10.6% presented a Healthy Diet. After the intervention, there was significant improvement in all classifications, and only one of the volunteers showed an inadequate diet classification. Diet quality classification observed in the studied population is presented in Figure 1.
The purpose of the study was to evaluate the effect of a short-term nutritional counseling program, on the diet quality and total energetic value in individuals with Metabolic Syndrome.
Food habits changes focused on MS should prioritize a healthy body weight reduction (2, 4). During this study the body weight reduction mean reached the 5% goal established (2, 4) compared to the beginning, and the mean weight changed from 87 kg to 82 kg at the follow-up ends. The proposed model showed a significantly reducing BMI, abdominal circumference, fasting insulin and glucose, triglycerides and systolic blood pressure (data not shown).
The HEI BR indicates it is a tool that assigns a score and ranks important dietary risk factors for MS. As suggested by other evidence, diets rich in salt, total fat and saturated fat intake are directly associated with chronics diseases, such as obesity, cardiovascular disease (CAD), hypertension and diabetes, all those intrinsically related to the Metabolic Syndrome's diagnostic criteria (8, 18).
The Healthy Eating Index was the instrument used by McCullough et al. (19) to assess the diet quality in cohort data studies such as Nurses’ Health Study and Professional’s Follow-up Study. The authors demonstrated that men with top HEI scores, which means a high quality diet, had 39% less risk to develop cardiovascular diseases if compared to those with a low score. In women, this ratio would determine 28% less risk of CAD for those with high diet quality scores when compared to the ones that presented low HEI scores (19). The nutritional intervention proposed by this model was shown to improve dietary items recommended by NCEP ATP III (4) and other health associations around the world (2, 4).
The final HEI BR score presented significant improvement in this population, which demonstrates the benefits of the nutritional behavior in these volunteers' diet quality. The mean score of the studied population's diet quality increased significantly, from 53.02 to 61.65, after intervention (p 0.000). This mean value was lower than that observed in other studies with American population (7, 8) and was similar to those observed in a recent study with Brazilian volunteers (20). The amount of individuals classified on an Inadequate Diet was six times smaller at the end of the monitoring phase. The amount of individuals classified on a Healthy Diet was four times higher, and the percentage of diets classified as Diet that Needs Change was 25% lower, when compared to the beginning of the study.
Among the components studied in the HEI BR the highest score means, i.e. the most adequate intake, was observed in the Cholesterol and Saturated Fat groups during both phases of the study. These results, also found by Fisberg et al (10), may be explained in the light of the inaccuracy of data regarding the quantity of these dietary items in the nutrition facts label and food labels.
The nutritional intervention performed led to an improvement in dietary components that had low scores before the study. Although the nutrition component Fruit had a significant score increase, from the lowest classification to the intermediate classification, this item still remained as the one with the lowest HEI mean for this population, a result that was similar to that reported by Fisberg et al. (20).
The nutritional intervention model resulted in a significant improvement in seven out of ten components that include HEI BR, and an unexpected score reduction regarding Grains group. These results emphasize the need for specific guidance about an adequate intake of this nutritional group. It is possible to hypothesize that this this nutritional group was underestimated during reports and dietary records (20).
The nutritional intervention performed promoted a significant increase in Total Fat, Saturated Fat and Sodium scores, which were items that presented low values in the beginning of the program. Previdelli’s et al. (21) reported a similar result for sodium components. There was also a significant improvement in the mean score for the following nutritional groups: Vegetables and Fruit, and Diet Variety. An adequate Fruit and Vegetable intake becomes important because of its relationship with abdominal obesity and cardiometabolic diseases increase, as shown in previous studies (18,19).
In 2005, Fung et al. (22) verified an association between scores provided by different diet quality and serum concentrations in inflammatory markers assessment tools. In that study, a high score in the adapted Healthy Eating Index was associated to a lower concentration of inflammatory biomarkers, endothelial disorder and a 30 percent reduction in C-reactive protein levels of those subjects who presented a higher dietary quality.
A meta-analysis verified that fruit and vegetable intake is inversely associated to the risk of developing CVD (23). In the present study, subjects with MS presented low scores regarding an adequate ingestion of Fruit and Vegetables groups. After completing the monitoring phase a significant increase was observed in these groups' scores, which demonstrates a more adequate dietary intake after the nutritional intervention.
To know the quality and the adequate intake of certain food items, i.e. individuals diagnosed with CAD, diabetes or hypertension, allows focusing the intervention on the dietary risk. The adoption of this tool should be stimulated mainly because it is cost effective and easy to understand, either by professionals or by the general population, and due to the gradient of dietary quality it reflects.
However, some limitations in this study should be mentioned, like the difficulty to get volunteers due to some demanding exclusion criteria, as follows: use of drugs for MS diagnosis criteria and dietary supplementation. During the research phase, more than one thousand people interested in participating contacted the researchers, but only 10 percent fulfilled the inclusion criteria.
Studies have shown a tendency to underreport food intake by female subjects, overweight individuals as well as by people who are undergoing treatment for weight loss (24). In the present study, most of the sample consisted of female subjects, and all participants were overweight or obese as of the process of reducing weight. These characteristics may indicate a possible underreporting of actual intake. Another limitation is linked to the methods of dietary surveys used. It is known that the information collected in the 24-h recall and food record depends of memory and the cooperation of the patient. However, these methods are a widely used to collect data on eating behaviors and measuring energy intake in adults (24).
HEI Adapted to Brazilians revealed a significant improvement in overall dietary quality, demonstrating that a short-term nutritional counseling program promoted a significant result in individuals with MS.
The associations found between HEI BR components and the studied variables suggest that nutritional intervention plays a positive role in changing risk factors present in MS. This study demonstrated nutritional intervention efficiency in seven out of ten HEI BR components, and contributes to devise intervention approach in clinical practice.
Other studies and models where dietary quality indexes are adapted become necessary to measure other dietary characteristics, such as the amount of trans fat, and to adjust sugar intake.
We thank to the participants for their valuable help. We thank Professor Helio Radke Bittencourt for statistical assistance. The authors had no conflicts of interest to declare.
Recibido: 04-04-2014
Aceptado: 11-06-2014