
Ecuador is undergoing a nutrition transition where overweight/obesity coexist with undernutrition. The objective of this study was to determine nutritional status, physical activity, fruit and vegetables consumption frequency among school-going adolescents in the canton of Paute and further explore if these variables were differential by urban vs. rural residence. We conducted a cross-sectional study using a random sample of students aged 12 to 19 years from the only two public secondary schools in the canton Paute. We determined nutritional status according to the World Health Organization criteria. Demographics, physical activity habits, fruit and vegetable consumption frequency were determined by questionnaires. Of the total of 314 students, 44.9% lived in urban area and 55.1% in rural area. The prevalence of overweight/obesity was significantly higher among students with urban vs. rural residence (28.4% vs. 17.9%; P=.03). The prevalence of stunting was significantly higher among students with rural vs. urban residence (31.8% vs. 16.3%; P=.002). There were no significant differences detected between groups in the frequency of consumption of fruits and vegetables. Urban residence was associated with a greater mean number of minutes of outdoor recreation after school (76.0 minutes vs. 57.1 minutes; P=.02), greater weekly hours of planned physical activity (2.0 hours vs. 1.6 hours; P=.007), and greater daily screen time in front of a television or computer (3.2 hours vs. 2.5 hours; P<.001). Interventions to prevent or reduce overweight/obesity in Paute and other similar areas with students from both urban and rural areas should consider place of residence in their design.
Key words: Adolescent; rural population; urban population; overweight; obesity; Ecuador.
Ecuador experimenta una transición nutricional donde el sobrepeso y la obesidad coexisten con la desnutrición. El objetivo de este estudio fue determinar estado nutricional, actividad física, consumo de frutas y verduras en adolescentes del cantón Paute-Ecuador y explorar las diferencias entre residencia urbana y rural. Se realizó un estudio transversal, con una muestra aleatoria de estudiantes de 12 a 19 años de edad en los dos únicos colegios de Paute. Se determinó el estado nutricional con el criterio de Organización Mundial de la Salud. Se determinó lugar de residencia, actividad física y frecuencia de consumo de frutas y verduras mediante cuestionarios. De los 314 estudiantes, 44,9% vivían en área urbana y 55,1% en área rural. La prevalencia de sobrepeso/obesidad fue más alta entre estudiantes del área urbana vs los del área rural (28,4% vs 17,9%; p=0,03). La prevalencia de talla baja fue mayor en área rural comparado con área urbana (31,8% vs 16,3%; p=0,002). No se encontraron diferencias significativas en el consumo de frutas y verduras. Los estudiantes del área urbana tuvieron un mayor promedio de minutos de actividad física después del colegio (76,0 vs 57,1 minutos; p=0,02), mayor número de horas de actividad física a la semana (2,0 vs 1,6 horas; p=0,007), y mayor tiempo frente a la pantalla del televisor o computador (3,2 vs 2,5 horas; p<0,001). Las intervenciones para prevenir o reducir el sobrepeso/obesidad en Paute y otras áreas similares con estudiantes de áreas urbana y rural deben considerar el lugar de residencia en sus diseños.
Palabras clave: Adolescentes; población rural; población urbana; sobrepeso; obesidad; Ecuador.
Facultad de Ciencias Médicas, Universidad de Cuenca, Campus Paraíso, Cuenca, Ecuador. Dirección de Investigación, Universidad de Cuenca, Ciudadela Universitaria, Cuenca, Ecuador.
Similar to other countries in Latin America, Ecuador is undergoing a nutrition transition where undernutrition and overnutrition co-exist (1). The most recent and only nationally representative data on the prevalence of overweight and obesity among adolescents in Ecuador come from the Ecuadorian Health and Nutrition Survey (Encuesta Nacional de Salud y Nutrición [ENSANUT] 2012, which reported an overall prevalence of overweight/obesity of 26.0% in adolescents (2). In ENSANUT, overweight/obesity was higher among younger (12-14 years) vs. older adolescents (15-19 years) (27.0% vs. 24.5%), higher among females vs. males (28.8% vs. 23.3%), higher among the wealthiest adolescents vs. the poorest adolescents (28.3% vs. 19.4%), highest among Afroecuadorians (43.7%), and highest among adolescents from the province of Azuay (34.4%) and the Galápagos islands (34.5%) (2). As elsewhere in Latin America (3), the prevalence of overweight/obesity among adolescents in Ecuador is higher in urban settings compared with rural settings (2, 4). In ENSANUT the prevalence of overweight and obesity in urban vs. rural environments was 29.4% vs. 21.1% in the sierra region, 28.9% vs. 19.4% in the coastal region, and 26.2% vs. 21.8% in the Amazon region (2).
At the same time, stunting remains an important public health issue, with 19.1% of the adolescent population stunted, with the highest prevalence in the indigenous population (48.8%), greatest prevalence in the poorest vs. wealthiest adolescents (33.8% vs. 6.7%), and rural vs. urban populations (sierra region 32.7% vs. 17.8%; coastal region 18.4% vs. 16.6%; Amazon region: 28.4% vs. 17.2%) (2).
Lifestyle factors are highly relevant to the prevalence of overweight/obesity in Ecuador. In terms of physical activity, only 28.0% of adolescents were classified as physically active in ENSANUT (defined as at least 60 minutes of daily moderate to vigorous physical activity for 5 out of the last 7 days) (2). Similarly, excessive screen time is an issue with 25.7% of adolescents watching 2 or more hours of TV or playing videogames (not inclusive of computer, tablet, or cellular phone time). Lifestyle factors are also important for noncommunicable disease risk in general. In particular, reduced fruit and vegetable consumption is a known modifiable risk factor for noncommunicable diseases (5). Nationally representative data from ENSANUT indicate that in Ecuador, the average consumption of fruits and vegetables insufficient at 183 g daily in the overall population, and at 168 g for males and 184 g for females in the adolescent age group (2).
As school-based interventions are an attractive way to promote health in the adolescent population, we sought to determine the epidemiology of nutritional status, physical activity, and fruit and vegetables consumption frequency among school-going adolescents in the canton of Paute, Ecuador. As Paute is a canton with both urban and rural areas, we sought to further explore if these variables were differential by area of residence.
This cross-sectional study enrolled adolescents from the only two public secondary schools in Paute (“Ciudad del Paute” and “26 de Febrero”) in July 2014. Paute is a canton in the province of Azuay located in the southern sierra region of Ecuador, northeast from the city of Cuenca with approximately 25 thousand inhabitants. Like other cantons, Paute is further subdivided into several parroquias (parishes), which are either urban (i.e., within the town center) or rural (i.e., outside of the town center). A random sample was taken from each school, based upon an estimated sample size of 314. Sample size was based on determining the prevalence of obesity and was calculated assuming an 8% prevalence of obesity, an alpha of 0.05, and a precision of 3%. All students between the ages of 12 and 19 years old were eligible. We obtained written informed consent from both the students and their parents. The ethics committee of the University of Cuenca approved this study.
Two nutritionists and a pediatrician conducted anthropometric measurements and interviews, with previous standardized training. Students were asked their birth date (converted to age in years and categorized as ≤13 years, 14 years, 15 years, 16 years, and ≥17 years), sex, and maternal and paternal education level (none, primary school, secondary school, or greater). Weight was measured using a calibrated digital scale (Health o Meter®) to the nearest 0.1 kg with the children wearing light clothing. Height was measured using a portable stadiometer (Seca®) with the participants not wearing shoes. Waist circumference was measured to the nearest 1 mm using a nonelastic flexible measuring tape (Seca®) midway between the lowest rib margin and the iliac crest after exhaling in a standing position. Weight, height, and waist circumference were measured twice and the average of the two values was used in our analysis. Nutritional status was defined using the 2007 World Health Organization (WHO) growth reference curves for children aged 5 to 19 years, using the SAS Macro provided by WHO (6). Weight status was categorized using body mass index (BMI)-for-age z-score using the following standard deviation (SD) cutoffs: below -2 SD (underweight), between -2 SD and +1 SD (normal weight), between +1 SD and +2 SD (overweight), and above +2 SD (obese). Height status was categorized using height-forage z-score using the following cut-offs: below -2 SD (stunted) and between -2 SD and +2SD (normal). The WHO criteria were used in our main analysis to allow comparability with ENSANUT, but we also used the 2012 International Obesity Task Force (IOTF) criteria. For IOTF, we used charts to identify a corresponding BMI of 2 at 18 years (defined as overweight/obese), using the student’s BMI, age (at 0.5 year intervals), and sex (7). Abdominal obesity was defined as having a waist circumference at or above the 90th percentile for age and sex, using the Mexican-American child and adolescent population from the US National Health and Nutrition Examination Survey (NHANES) III as a reference group (8). Urban residence was defined as living in the city center of Paute and rural residence was defined as living outside of the city center, and determined based upon the participants’ self-reported residence.
Physical activity habits were assessed using an adapted questionnaire asking about sedentary and physical activity, developed in Chile and previously used to evaluate physical activity in school children in Cuenca, Ecuador (9). Students were asked how many hours they normally sleep at night and during the day; how many hours they spend inactive in class, doing homework or studying, during meals, in car or other transport, in front of television or computer or playing videogames; how many minutes a day of outdoor recreation outside of school (e.g., bicycling, playing soccer, running etc.); and how many hours per week in planned physical activity (e.g., gymnasium, soccer club, etc., including physical education classes at school).
Fruit and vegetable consumption was assessed by a questionnaire asking about the number of typical daily servings of each. Nutritionists met with small groups of participants (approximately 5 students at a time) and went through the questionnaire, using photos and food models to explain serving sizes. Specific fruits included bananas, apples, peaches, papaya, pineapple, grapes, oranges, tangerines, and tomate de árbol (tamarillo). Specific vegetables were lettuce, cauliflower, cabbage, tomato, beets, cucumbers, and carrots. In addition to the mean number of servings for each food group, fruit and vegetable consumption was dichotomized into ≥5 daily servings and <5 daily servings, consistent with recommendation from WHO (at least 400 g daily, excluding potatoes and tubers) (10).
We first describe the overall sample by demographics, nutritional status, physical activity habits, and fruit and vegetable consumption frequency. We then used Pearson’s Chi-Square tests to evaluate the distribution of categorical variables by urban vs. rural residence status. Fisher’s exact test was used for any variables with counts <5. For continuous variables, Mann-Whitney-Wilcoxon tests were used to compare means by residence status. An alpha value <0.05 was considered to be statistically significant. All analyses were performed in SAS 9.3 (SAS Institute, Cary NC).
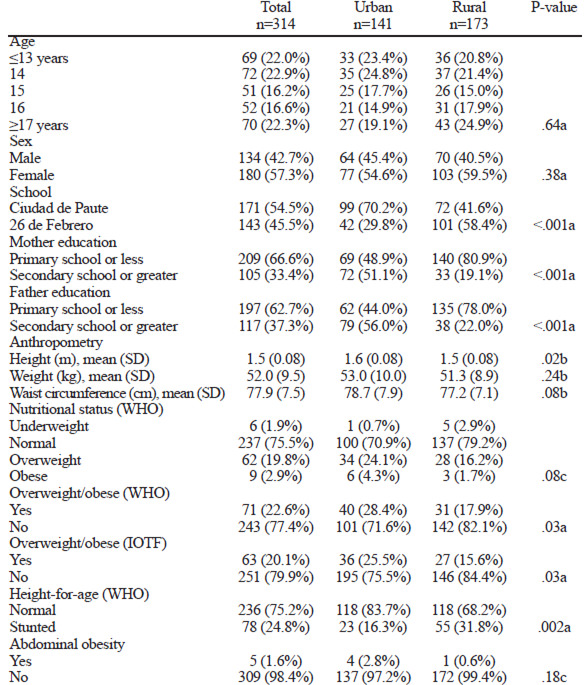
Overall, 314 students were enrolled and completed this study. There were more female than male students (57.3% vs. 42.7%) and most were 16 years old or younger (77.7%). Approximately two-thirds of participants’ mothers and fathers had an education level of primary school or less (66.6% and 62.7%, respectively). With regard to nutritional status (WHO criteria), 1.9% of students were underweight and 22.6% (95% confidence interval (CI): 17.9%, 27.6%) were overweight/obese with 2.9% (95% CI: 0.9, 5.0) obese. In addition, 1.6% of had abdominal obesity and 24.8% were stunted. When stratifying by sex, there were no significant differences detected for overweight/obesity (males 23.9% vs. females 21.7%; P=.64) and stunting (males 28.4% vs. females 22.2%; P=.21), using the WHO criteria.
When comparing demographics and anthropometry by residence (Table 1), students with rural residence significantly more often had parents with an education of primary school or less (mothers: 80.9% vs. 48.9%, P<.001; fathers: 78.0% vs. 44.0%, P<.001), were less often overweight or obese (17.9% vs. 28.4% P=.03), and were more often stunted (31.8% vs. 16.3% P=.002), using the WHO criteria, compared with students with urban residence. In our sensitivity analysis re-defining o v e r w e i g h t / o b e - sity per the IOTF criteria, the overall prevalence of overweight/obesity diminished (WHO: 22.6%; IOTF: 20.1%); however, overweight/obesity remained more prevalent in urban vs. rural areas (IOTF: 25.5% vs. 15.6%, P=.03).
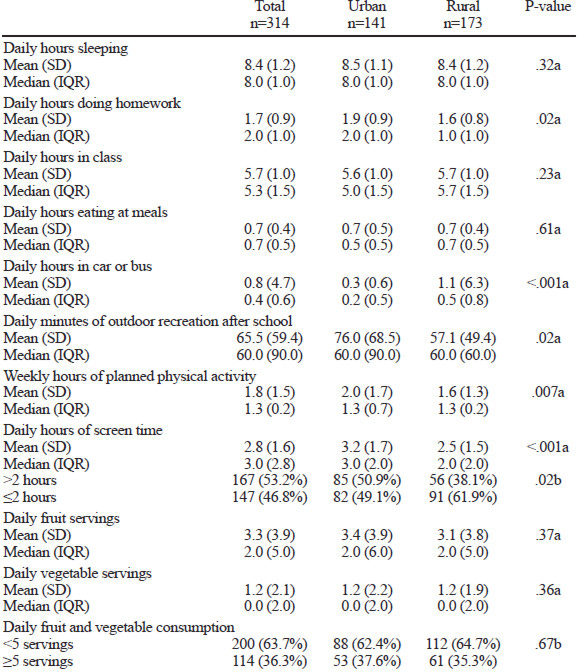
When comparing physical activity habits and fruit and vegetable consumption frequency by residence (Table 2), students with rural residence spent fewer hours doing homework daily (1.6 vs. 1.9; P=.02), spent more hours in a car or bus daily (1.1 vs. 0.3; P<.001), had fewer daily minutes of outdoor recreation outside of school (57.1 vs. 76.0; P=.02), had fewer weekly hours of planned physical activity (1.6 vs. 2.0; P=.007), and had fewer hours of screen time (2.5 vs. 3.2; P<.001), compared with students with urban residence. The majority of students had <5 servings of fruits and vegetables daily, but there were no significant differences detected between urban and rural groups.
In Paute, we found that the prevalence of overweight and obesity among adolescents was numerically lower than the national prevalence (22.6% vs. 26.0%); however, the prevalence of overweight/obesity surpassed national prevalence in students with urban residence (28.4%). Additionally, the prevalence of overweight/obesity was substantially lower than what was reported by ENSANUT specifically for the prevalence of Azuay (22.6% vs. 34.4%). The prevalence of stunting was higher in Paute compared with the national prevalence in adolescents (24.8% vs. 19.1%) and was particularly high in adolescents with rural residence (31.8%). We found significant differences between the prevalence of overweight/obesity and stunting when comparing urban and rural residence; urban students were more often overweight/obese and less often stunted and rural students were less often overweight/obese and more often stunted.
In Ecuador, the WHO reference values are most frequently used for clinicial practice and research (2). In this study, we included the IOTF criteria strictly for the purpose of comparison, as it has previously been used in other research in Ecuador (4). In our analysis using the IOTF classification of overweight/obesity, there was lower prevalence of overweight/obesity overall compared with the WHO criteria; however, the distribution of overweight/obesity by urban vs. rural residence was similar. This variability in overweight/obesity prevalence by different definition was also observed in a study of school-aged children in Cuenca, Ecuador (9). This highlights the potential value in exploring the need for country specific reference values for Ecuador, as has been done in Bolivia (11). Aside from overweight/obesity, this study also emphasizes the high prevalence of stunting is in Ecuador, particularly among students with rural residence in Paute. In Ecuador and in other places with a high prevalence of stunting, adequate nutrition needs to be addressed as early as possible in the life course, as this clearly affects health and wellness, but can also impact later school performance, which can ultimately lead to missed opportunities in education to improve living conditions for them and their families in the future (2).
Our findings of greater prevalence of overweight/obesity among urban adolescents are consistent with both ENSANUT (2) and a previous cross-sectional study, which compared adolescents from the urban city of Cuenca with the mostly rural canton of Nabón, both in Azuay province (4). Although there are few studies exploring this phenomenon, the higher prevalence of overweight/obesity among adolescents with urban vs. rural residence is consistent with studies from Brazil (3), India (12), and Nigeria (13). A factor that may at least partially explain the higher prevalence of overweight/obesity in urban adolescents is higher socioeconomic status. Although we did not measure socioeconomic status in our study, urban students had parents with significantly higher education level, which may be associated with greater economic prosperity. This phenomenon is similar in other low- and middle-income countries, and may be explained by greater economic power to buy high energy density foods and drinks and access to items that promote a more sedentary lifestyle (14). However, we cannot be certain about this in Paute, given that we did not collect data on pocket money, socioeconomic status, or access to high energy density foods.
In our study, urban adolescents appeared to be more physically active despite greater screen time, based on their reports of programmed physical activity and after-school recreation. This finding is consistent with a previous study comparing Cuenca and Nabón in Ecuador reported that urban dwelling adolescents from Cuenca had greater physical fitness (15). However, physical activity questionnaires that have been used in studies comparing urban and rural adolescents have generally had suboptimal validity for rural students, in Ecuador (16), and in other parts of the world, such as in Vietnam (17). In areas like Paute with students of mixed urban and rural residence, questionnaires to measure physical activity need to take into account the different built environments of the population and associated activities (e.g., participating in farming) in order to get an accurate estimation of different measures of physical activity. This is an important area for future research.
Although we did not detect significant differences by residence in terms of fruit and vegetable consumption frequency, the distribution of these frequencies highlights some potential areas for intervention. In particular, vegetable consumption had a skewed distribution, with a median of 0 daily servings (interquartile range of 2 servings), indicating deficient intake in the majority of students. In contrast to vegetable consumption, fruit consumption was higher with a median of 2 daily servings (interquartile range of 5 servings). However, when combining these variables, fruit and vegetable consumption was deficient in most students, with 63.7% eating less than 5 servings daily (approximately 400 g), as recommended by WHO. Similar trends have been observed at the national level with average consumption of fruits and vegetables <200 g for adolescents (2). This is an ideal area for health promotion, which is facilitated by the abundance and low price of fruits and vegetables in many areas of Ecuador and particularly in Paute. This is a major advantage over many countries, particularly in North American and Europe, where fruits and vegetables are expensive (18) and a socioeconomic gradient for fruit and vegetable consumption exists (19). Increasing fruit and vegetable consumption needs to be a public health priority in Ecuador in order to reduce the burden of noncommunicable disease (5, 20), and could be achieved through implementing a national campaign with a simple core message to increase fruit and vegetable consumption, as has been done in the United States (21).
There are some limitations of this study that should be considered. First, in terms of the survey design, the frequency of fruit and vegetable consumption was limited to the specific items included in the survey and may not have been all-inclusive, and all data were self-reported and thus, potentially subject to bias. Second, our main analysis was powered to estimate the prevalence of obesity in Paute and thus, we may have had insufficient power to detect differences of some variables when comparing by residence. Third, we did not control for confounders that may have at least partly explained some of the associations we observed; however, the objective of this study was to simply look at distributions of variables by area of residence. Analysis of adequately powered, nationally representative surveys with more detailed data would be best to clarify pathways in which area of residence influences nutritional status. Although our results are only generalizable to adolescents who attend public school in Paute, some of our findings are relevant for similar communities in the region.
The high prevalence of co-existing overweight/obesity and stunting in Paute exemplifies the nutrition transition in Ecuador. Our findings suggest that school-based interventions to reduce overweight/obesity in Ecuador need to consider students’ residence in the design and implementation of interventions, at least in schools with a mix of urban and rural students. Based on our findings, we would propose school-based interventions in Paute and similar areas focus on increasing fruit/vegetable consumption, reducing screen time in all students, but particularly in urban students, and increasing out-of-school physical activity in all students, but particularly in rural students. In addition, future research is needed to identify additional risk factors that may explain why overweight/obesity is more prevalent in urban adolescents compared with rural adolescents from the same region in Ecuador and in other countries in nutritional transition.
We would like to thank the students who participated in this study, as well as the secondary schools (“Ciudad del Paute” and “26 de Febrero”) for their collaboration. We would also like to thank nutritionists Diana Morales and Gabriela Molina for their contributions in carrying out this study.