Introduction
Meeting pregnancy micronutrients requirement through diet alone remains challenging, as dietary patterns often do not change during this period. Deficiencies in key micronutrients such as iron, calcium, folic acid, vitamin D, and copper persists even in populations with adequate food access (1,2), and are exacerbated by the high prevalence of unplanned pregnancies (3,4), This underscores the importance of preconception micronutrient status for pregnancy outcomes (5,6), as well as its influence on infant health during early life, given the limited bioavailability of some micronutrients such as iron and iodine in breast milk (6). From a Developmental Origins of Health and Disease (DOHaD) perspective, nutrition during preconception and pregnancy is critical for fetal development and long-term health, with suboptimal maternal micronutrient status linked to increased risk of chronic non-communicable diseases later in life (5).
Latin America continues to face a high burden of micronutrient inadequacy among women of childbearing age (WCA) despite fortification and supplementation programs. Anemia remains prevalent, and intakes of key micronutrients as calcium, vitamin D, vitamin E, choline, and long-chain omega-3 fatty acids are persistently low (7–10), coexisting with excess sodium intake and increasing overweight prevalence. Micronutrient adequacy is strongly influence by socioeconomic and behavioral factors, particularly dietary diversity, a key predictor of micronutrient adequacy in WCA (11–13), highlighting the need to evaluate whether prenatal supplementation effectively addresses population-specific nutritional gaps (14).
Population-level interventions, such as folic acid fortification, have demonstrate success in reducing neural tube defects (15,16), however, the implementation of WHO multiple micronutrient supplementation (MMS) recommendations has been slow in the region (17). Given that preconception nutritional status underpins pregnancy outcomes and dietary patterns trend to persist during gestation (17), there is a need to evaluated whether current prenatal supplements adequately address documented nutrient gaps (6,14,18). This study aimed to evaluate the micronutrient composition of commonly prescribed prenatal supplements in the ELANS countries and compare them with dietary intake and dietary diversity reported for WCA to identify gaps relevant for public health interventions.
Materials and methods
The ELANS study was designed as a cross-sectional, multicenter, household-based survey conducted between 2014 and 2015 in eight Latin American countries: Argentina, Brazil, Chile, Colombia, Costa Rica, Ecuador, Peru and Venezuela. Its primary objective was to assess dietary patterns and micronutrient adequacy among urban residents aged 15-65 years. A multistage, stratified random sampling design was applied, ensuring representation by geographic region, sex, age, and socioeconomic status, with a maximum sampling error of 3.49% at a 5% significance level. From a total of 9,218 participants, this analysis included 3,704 non-pregnant, non-lactating women of childbearing age (15-49 years) (19), to characterize usual preconception micronutrient intake.
Dietary intake data was assessed using two non consecutive 24-hour dietary recalls administered up to eight days apart and distributed across weekdays and weekends to capture intra-individual variability. Trained interviewers applied the United States Department of Agriculture’s (USDA) five-step multiple-pass method, and portion sizes were estimated using country-specific photographic atlases and standardized household measures. Foods items were coded and linked to the Nutrition Data System for Research (NDS-R 2014), which provided estimates of energy and nutrient intake. Usual intake distribution was estimated using the Multiple Source Method (MSM) (https://msm.dife. de/tps/en), developed within the European Prospective Investigation into Cancer and Nutrition (EPIC) to adjust for within-person variability. Micronutrient intake were energy-adjusted (expressed per 1000 kcal) to account for total energy intake and reduce potential bias from misreporting (18,20).
Dietary diversity was assessed based on the number of food groups consumed, with the intake of five or more food groups indicating a diverse diet. This indicator was used to characterize dietary patterns and vulnerability to micronutrient inadequacy among WCA (7). For the supplementation analysis, scenarios were applied uniformly across the population to reflect routine clinical practice, in which prenatal supplements are typically prescribed at fixed doses regardless of individual dietary diversity. The potential differential effects of supplementation according to dietary diversity are acknowledged as a study limitation.
Information on prenatal supplementation was obtained from each ELANS country’s Principal Investigator (PI), who identified the most commonly prescribed supplements based on experts’ clinical practice (Supplement 1). The micronutrient composition and dosage of each supplement were verified using product labels and official technical datasheets. Supplement formulations varied across the countries, reflecting differences in product composition and dosing.
The analytical approach for supplement evaluation was adapted from DeSalvo el al. (21). Mean usual micronutrient intake derived from the ELANS dataset (7) was combined with the micronutrient composition of a representative prenatal supplement for each country, modeling a population-level supplementation scenario rather than individual intake. Total micronutrient intake (diet plus supplementation) was compared with Estimated Average Requirements (EARs), Adequate Intakes (IAs), and Tolerable Upper Intake Levels (Uls), when available, to estimate the proportion of women meeting recommendations and those potentially exceeding Uls under a daily supplementation. The model assumes full adherence to daily supplement use at recommended dosage. Supplement-derived nutrients were not energy-adjusted, and no assumptions were made regarding bioavailability across countries. These assumptions, while allowing standardized comparation, may not reflect real-world supplementation practices and are acknowledged as study limitation.
All procedures were approved by the Western Institutional Review Board (protocol #20140605) and by local ethics committees in each participating country. All participants provided written informed consent prior to data collection (22).
Results
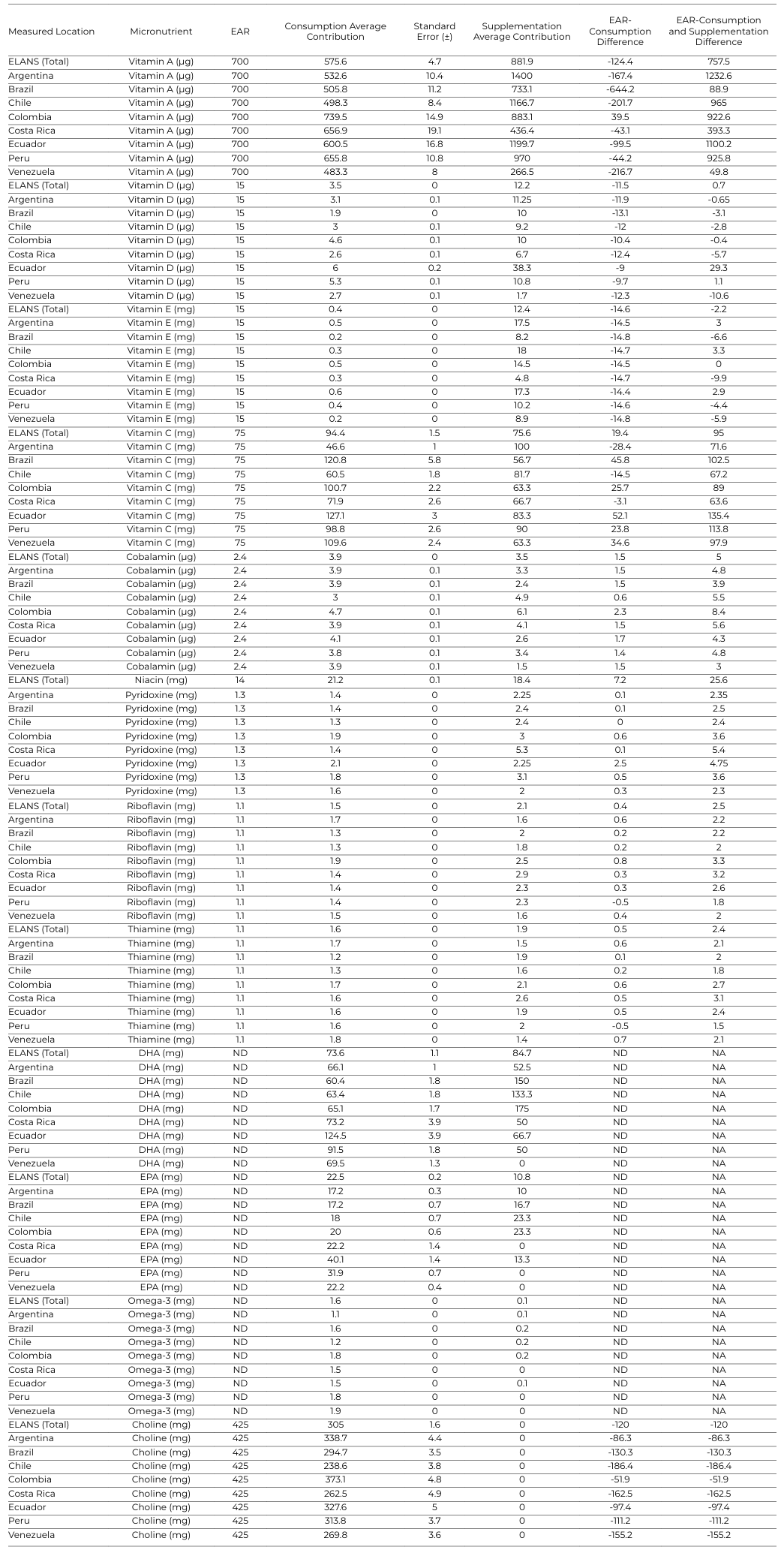
Detailed country-specific results for micronutrient intake are presented in Supplementary Tables 2, 3 (processed data) and Supplementary Tables 4, 5 (raw means and standard errors), with the key findings illustrated in Figures 1–7.
Prenatal supplement formulations show substantial variability across ELANS countries particularly in the content of key micronutrients as iron, calcium, magnesium, long-chain omega-3 fatty acids, and fat-soluble vitamins.
1. Minerals
Calcium. Mean dietary calcium intake was 542.5 mg (54.3% of recommendations), increasing to 66.5% with supplementation, remaining bellow adequacy in all countries. At the country level, supplementation improved intake but did not meet recommendations. Higher coverage was observed in Argentina, Colombia, and Ecuador (approaching approximately 85%), while Venezuela reached 67.9%. In contrast, Chile, Peru, Brazil, and Costa Rica remained below 65% even after supplementation (Figure 1).
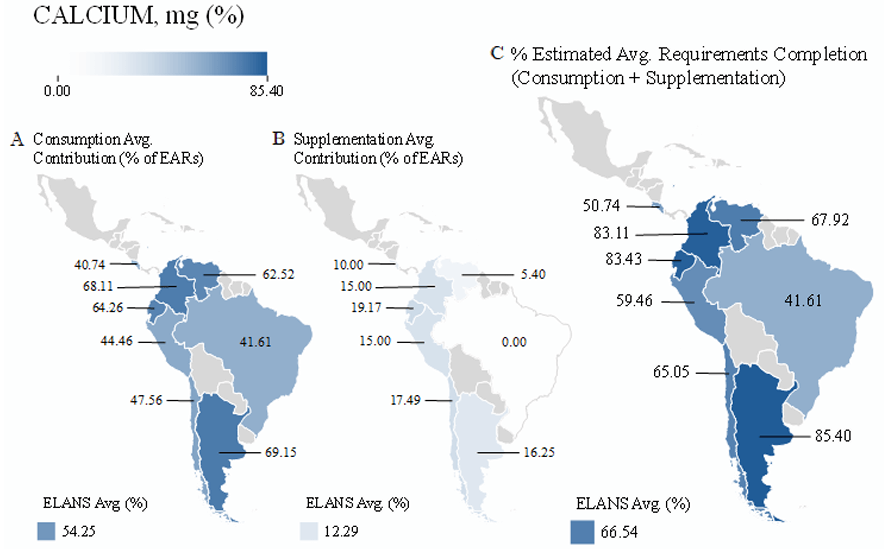
Figure 1. A) Average dietary calcium intake, (B) Contribution provided by the most consumed supplements per country, and combined values expressed as a percentage of (C) Estimated Average Requirements (%EARs)
Iron. Mean dietary iron intake was 12.3 mg (68.3%), increasing to 263.3% with supplementation, exceeding recommended levels and the tolerable upper intake level (UL).
Although dietary intake varied (50.0% in Brazil to 83.9% in Colombia), total intake surpassed recommendations in all countries, ranging from 163.3% in Venezuela to 463.9% in Argentina, reflecting substantial variability supplement composition (Figure 2).
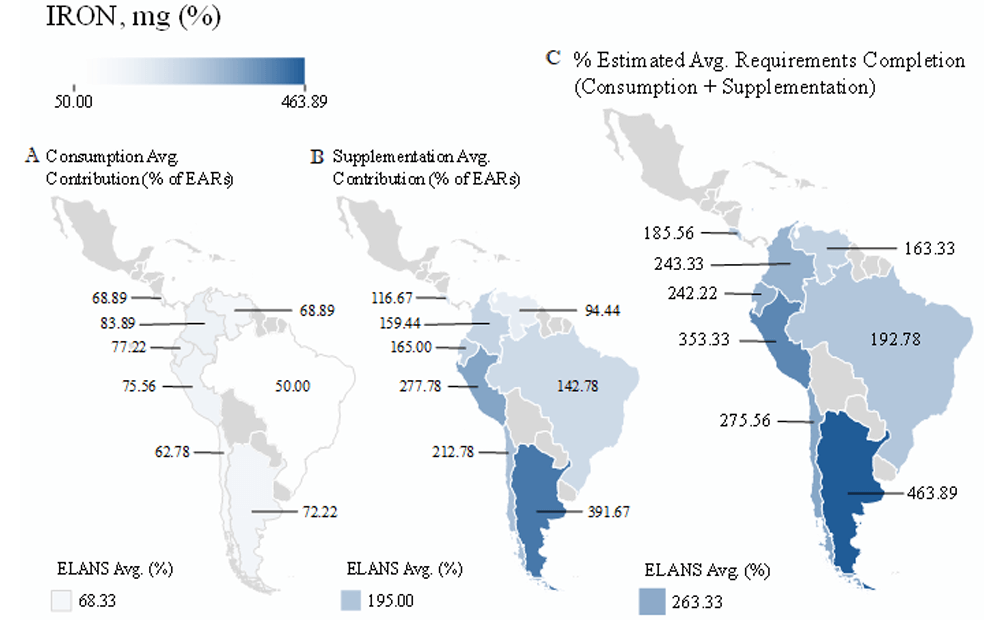
Figure 2. A) Average dietary iron intake, (B) Contribution provided by the most consumed supplements by country, and combined values expressed as a percentage of (C) Estimated Average Requirements (%EARs)
Magnesium. Dietary intake averaged 220.8 mg (84.9%), reaching 104.7% with supplementation. Supplement contribution varied widely across countries, with no inclusion in supplementation in Costa Rica and the highest contribution observed in Argentina (Figure 3).
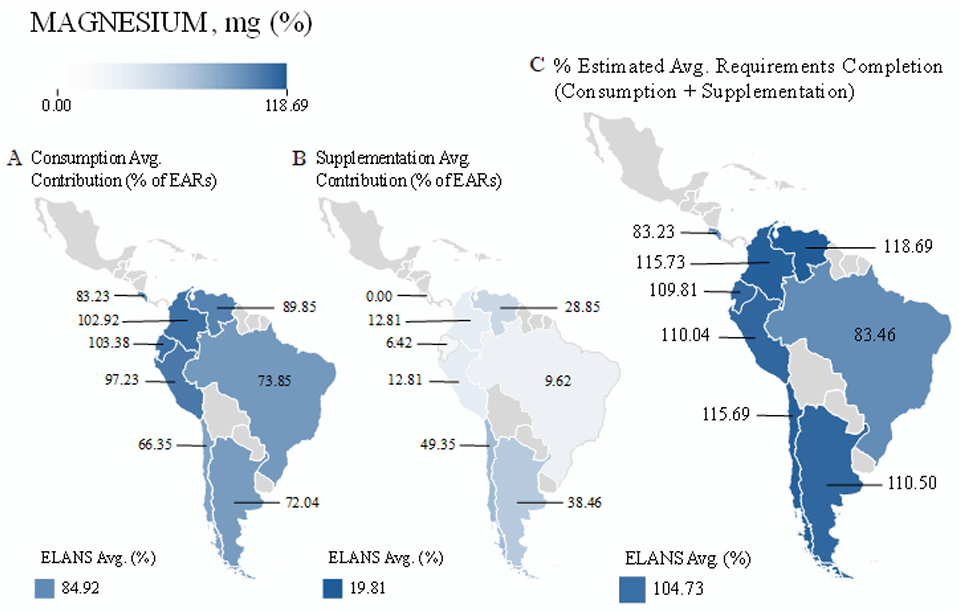
Figure 3. (A) Average dietary magnesium intake, (B)Contribution provided by the most consumed supplements by country, and combined values expressed as a percentage of (C) Estimated Average Requirements (%EARs)
Zinc, phosphorus, copper, and selenium. Dietary intake of these minerals exceeded recommended levels across the region and increase further with supplementation. Zinc reached 338.2% of recommendations with supplementation, phosphorus increase slightly from 167.9% to 172%, and copper rose from 200% to 271.4%. Selenium intake was already high from diet alone (241.6%) without supplementation.
Overall, supplementation further increased already excessive intakes, approaching or exceeding ULs and increasing potential health risk (Figures 4-5).
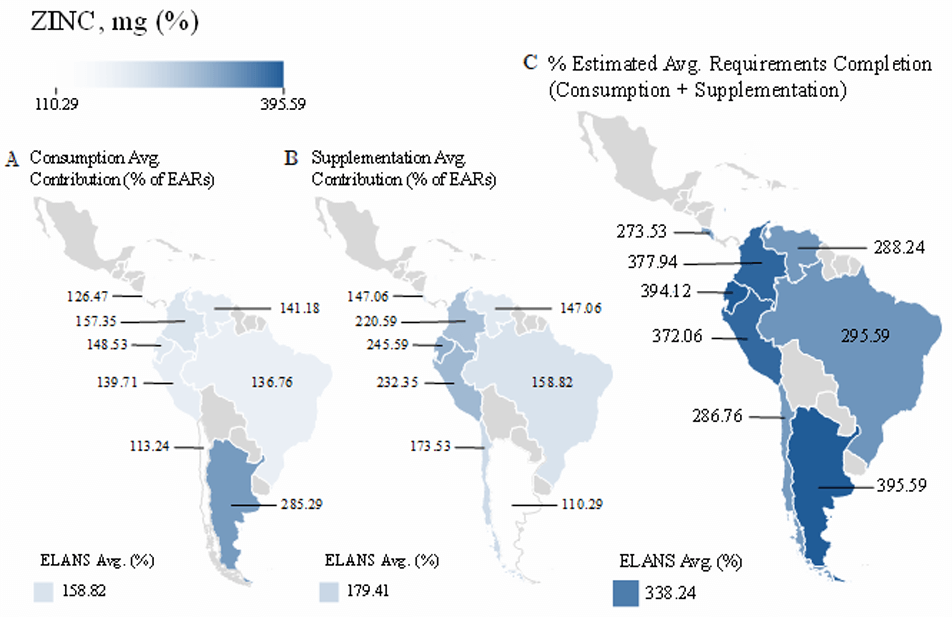
Figure 4. (A) Average dietary zinc intake, (B) Contribution provided by the most consumed supplements by country, and combined values expressed as a percentage of (C) Estimated Average Requirements (%EARs).
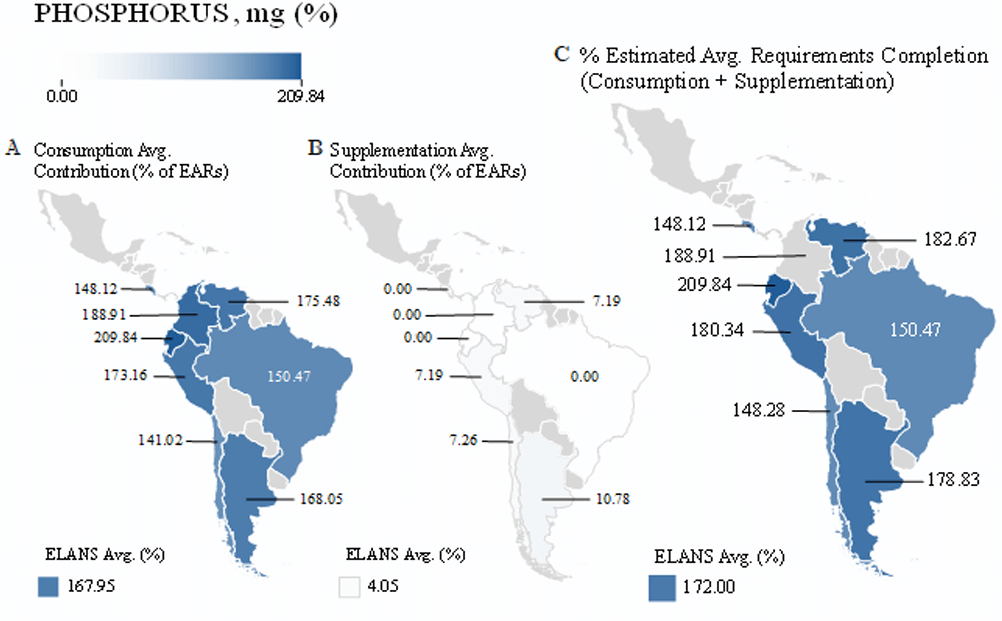
Figure 5. (A) Average dietary phosphorus intake, (B)Contribution provided by the most consumed supplements per country, and combined values expressed as a percentage of (C) Estimated Average Requirements (%EARs).
2. Fat‑soluble vitamins
Vitamin A. Mean dietary intake was 575.6 µg (82.2%), increasing to 208.2% with supplementation and exceeding the UL. Only Colombia met requirements through diet alone, while Chile showed the lowest intake. Supplementation resulted in excessive intake across all countries.
Vitamin D. Dietary intake was low (3.5 µg; 23.3%), but increased to 104.7% with supplementation. Intake varied across countries, and was higher in Ecuador, Peru, and Colombia, and lower in Brazil and Costa Rica.
Vitamin E. Mean dietary intake was minimal (0.4 mg; 2.7%), rising to 85.3% with supplementation. Adequacy was achieved in some countries (Chile, Argentina, Ecuador, and Colombia), but intake remained insufficient in Peru, Venezuela, Brazil, and Costa Rica.
3. Water‑soluble vitamins
Vitamin C. Mean intake was 125.9 mg (100.8%), indicating overall adequacy, although Costa Rica, Chile, and Argentina remained below recommendations. Supplementation increased intake above recommended levels across all countries.
B‑complex vitamins. Dietary intake was already high for all B vitamins, including cobalamin (162.5%), niacin (151.4%), pyridoxine (123.1%), riboflavin (136.4%), and thiamine (145.5%). Supplementation further increased total intake, exceeding 280% of recommendations across these vitamins (Figure 6).
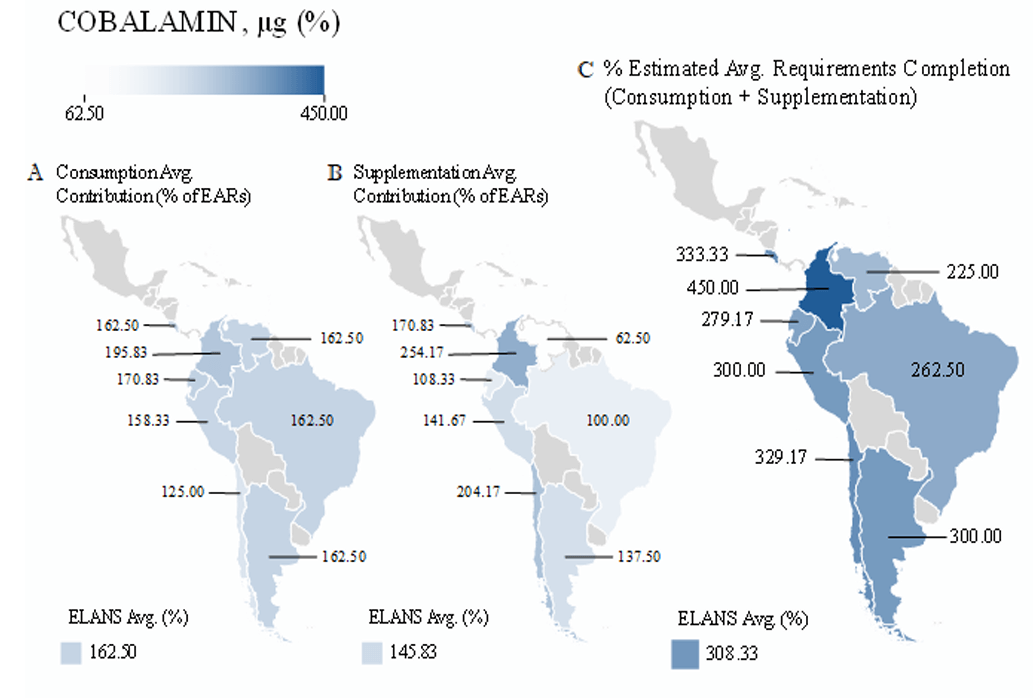
Figure 6. (A) Average dietary cobalamin intake, (B) Contribution provided by the most consumed supplements per country, and combined values expressed as a percentage of (C) Estimated Average Requirements (%EARs)
4. Other compounds
DHA, EPA, and omega‑3 fatty acids. Intake of long-chain omega-3 fatty acids (DHA and EPA) was quantified, although no reference values for adequacy were applied. Prenatal supplements contributed relevant amounts, substantially increasing total intake.
Choline. Mean dietary intake was 305 mg (71.8% of recommendations), with no contribution from prenatal supplements. Intake was lowest in Chile and remained below recommendations across all countries (Figure 7).
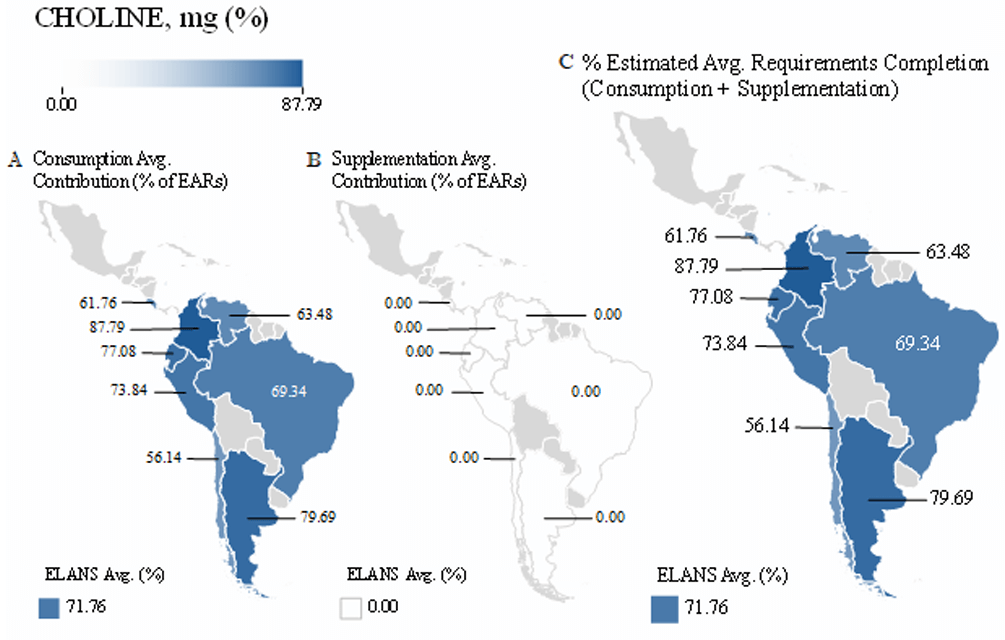
Figure 7. (A) Average dietary choline intake, (B) Contribution provided by the most consumed supplements per country, and combined values expressed as a percentage of (C) Estimated Average Requirements (%EARs).
Overall findings. Across ELANS countries, multiple micronutrient inadequacies were identified from diet alone, particularly for calcium, vitamin D, vitamin E, and choline. While prenatal supplementation improved intake for several nutrients, it frequently resulted in excessive intake, especially for iron, vitamin A, zinc, and B-complex vitamins. These findings highlight the coexistence of nutrient deficiencies and potential risk of excessive intake under current supplementation practices.
Table 1. Composition of most commonly prescribed prenatal supplements by ELANS country
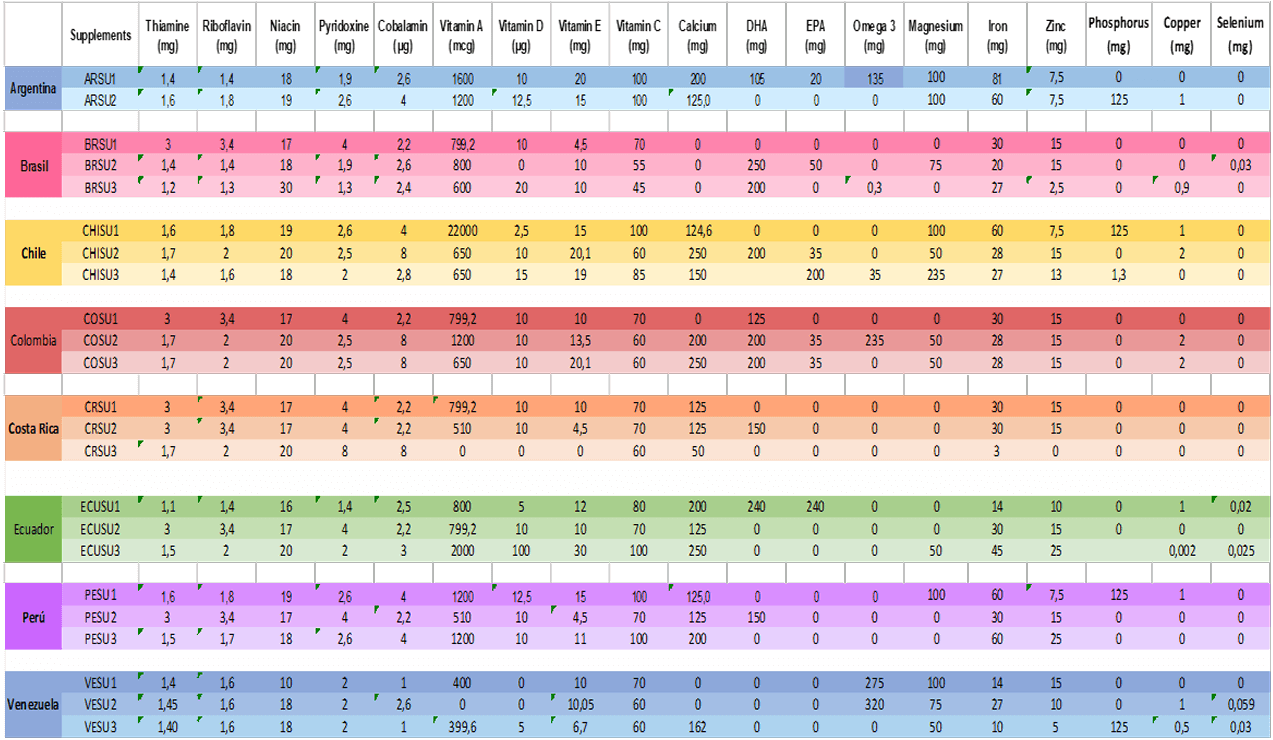
Table 2: Micronutrient Consumption, Supplementation, and Total Coverage as a Percentage of EARs
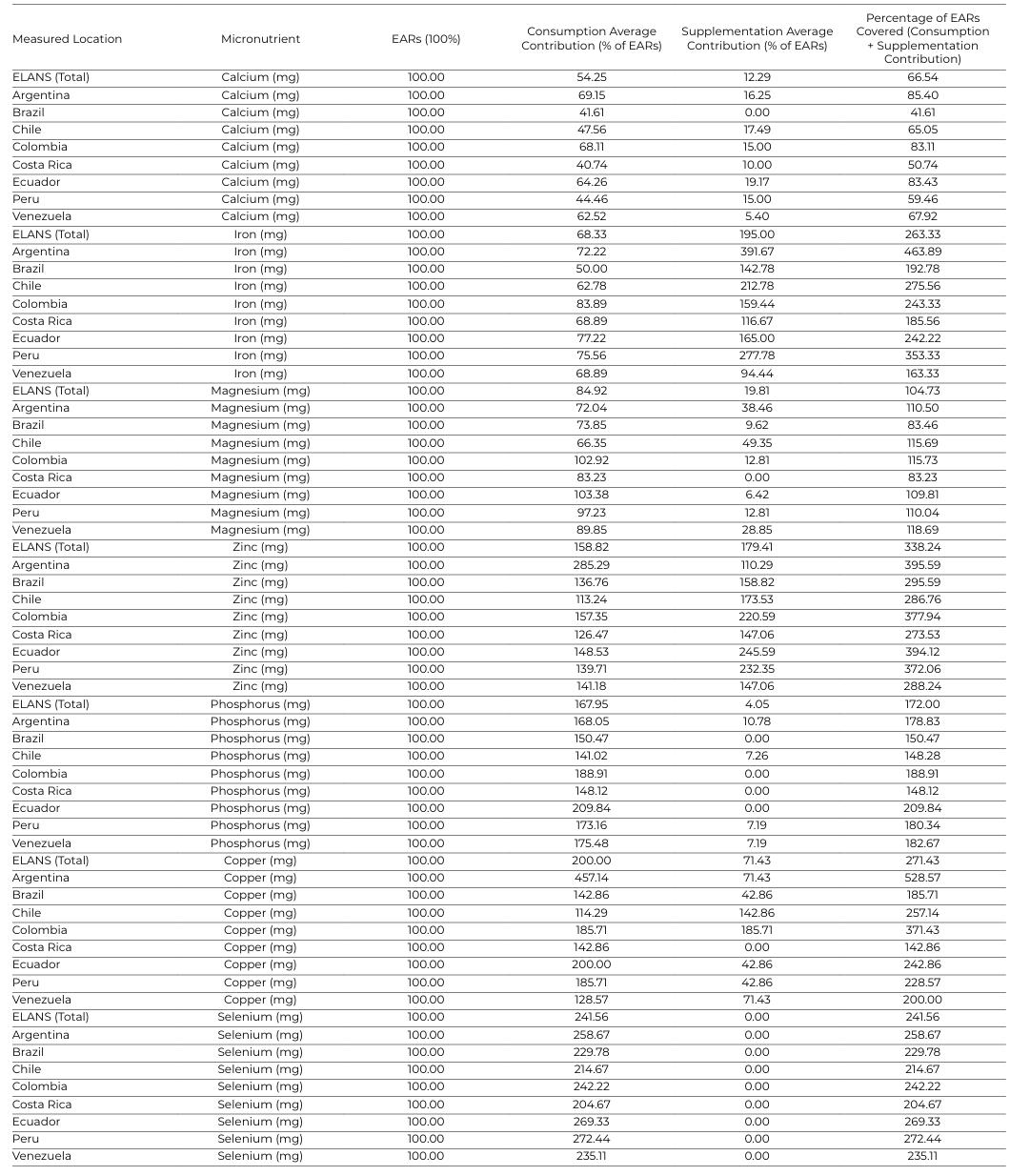
Table 3: Micronutrient: Consumption, Supplementation, and Total Coverage as a Percentage of EARs
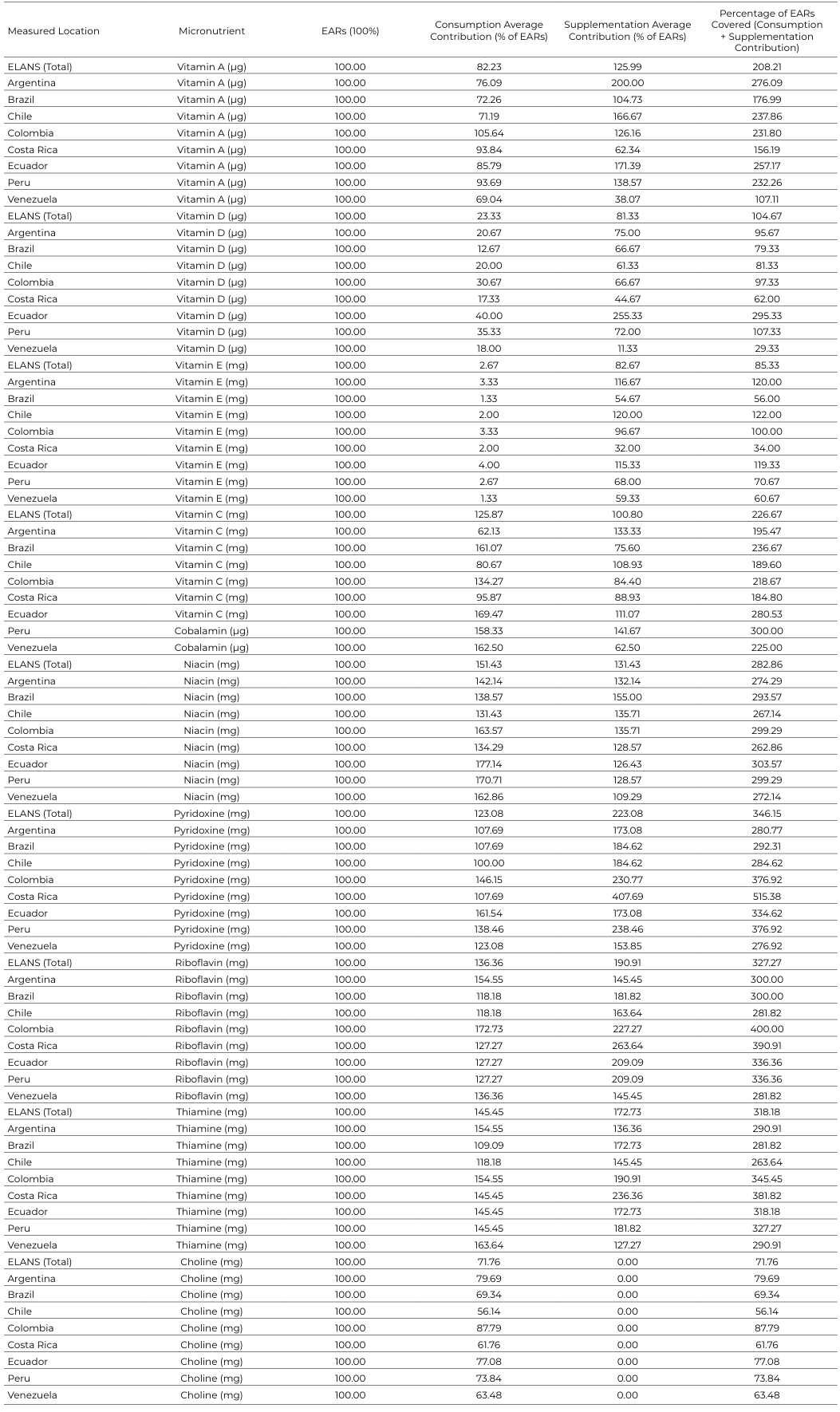
Table 4: Average Micronutrient Consumption, Supplementation, Standard Error, and EAR Differences
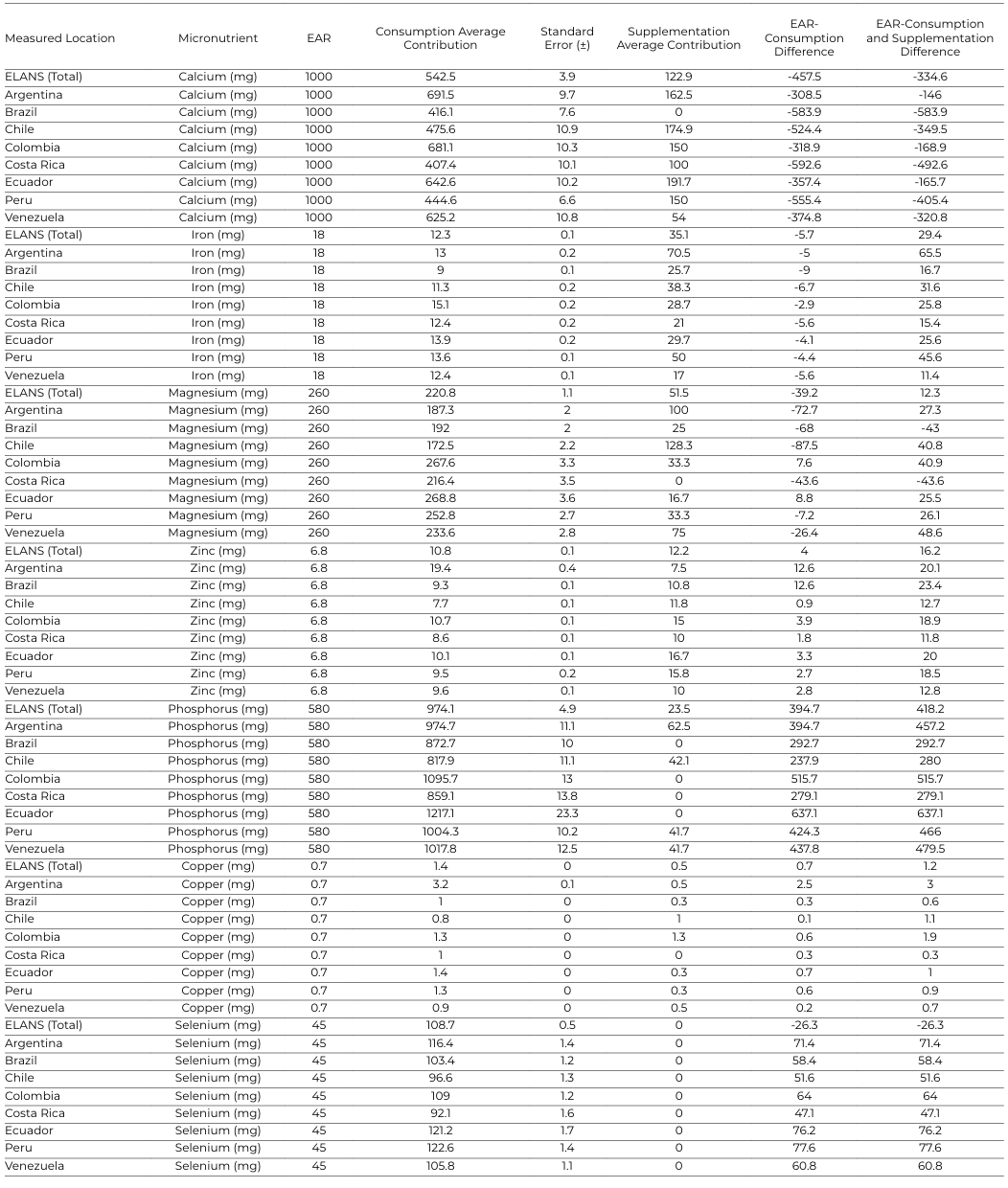
Table 5: Average Micronutrient Consumption, Supplementation, Standard Error, and EAR Differences
Discussion
The ELANS region exhibits a heterogeneous nutritional profile among women of childbearing age, characterized by persistent inadequacies in several essential micronutrients. Despite variability across countries, the overall pattern reflects suboptimal intake at the regional level, consistent with global evidence linking micronutrient deficiencies to socioeconomic inequalities, limited dietary diversity, and structural barriers to healthy diets (19,20,23,24).
Maternal nutrition during the preconception, pregnancy, and lactation periods plays a central role in perinatal outcomes and in shaping long term metabolic, immune and neurodevelopmental trajectories, in line with the Developmental Origins of Health and Disease (DOHaD) framework (5). In addition, dietary patterns tend to remain stable without interventions addressing social, behavioral, and environmental determinants (18,20).
These findings raise key questions for public health and clinical practice regarding the need for supplementation, priority micronutrients, and population-specific dosing strategies. Variability in dietary patterns further complicates these decisions, as nutrient requirements may differ according to dietary models (e.g. plant-based diets), underscoring the need for context-specific approaches (25). Addressing these challenges requires harmonized data systems that integrate dietary intake and supplementation to evaluate their combined contribution to micronutrient adequacy (18).
Evidence from large-scale fortification programs in Latin America provides valuable insights into effective interventions. Mandatory folic acid fortification in countries such as Chile and Argentina have significantly reduced neural tube defects, demonstrating that population-level, evidence-based policies (16,26,27). These findings highlight the potential of regulatory strategies to address nutritional gaps that are difficult to overcome through individual behavior alone, suggesting that similar approaches could be extended to other key nutrients, including iron, vitamin D, and calcium (28).
Socioeconomic factors strongly influence dietary diversity and access to nutrition-related information, thereby affecting micronutrient adequacy. Evidence from low- and middle-income countries shows that lower income, limited educational, and reduced dietary diversity are consistently associated with inadequate micronutrient intake among WCA [24,29). These structural determinants underscore the need for integrate strategies combining supplementation with improved dietary diversity and nutrition education.
The ELANS findings confirm global evidence of inadequate intake of key “neuro-skeletal” nutrients. Intakes of vitamin D and vitamin E remain particularly low, while calcium intake is persistently insufficient, even with supplementation 7,9). These deficiencies are concerning given their roles in fetal organ development, bone health, and neurodevelopment, as well as in epigenetic and metabolic programming during critical periods (5). Although supplementation improves intake for some nutrients, it does not fully correct these deficits, highlighting a mismatch between supplement composition and population needs (5). In contrast, nutrients such as zinc, selenium, and several B-complex vitamins already exceed recommended levels through diet alone and may reach excessive levels with supplementation.
Iron represents a particularly complex case. Although intake appears relatively adequate at the population level, this may not reflect physiological status due to differences in bioavailability, dietary sources, and increased requirements associated with menstrual losses. The coexistence of apparently adequate intake with high anemia prevalence in the region underscores this limitation (8). Globally, nearly one-third of women are affected by iron-deficiency anemia (30), and intake-based assessments alone may not reflect true nutritional status (31,32). While supplementation can improve biomarkers such as hemoglobin and ferritin (33), combined intake from diet and supplements may exceed tolerable limits, emphasizing the need for more individualized, bioavailability-informed strategies (8,13).
Importantly, this study identifies a clear mismatch between prenatal supplement formulations and actual nutritional needs. While supplementation improves intake of some deficient nutrients, such as vitamin D, it frequently leads to excessive intake of others, including iron, vitamin A, and B-complex vitamins, while key nutrients such as calcium, vitamin E, and choline remain insufficient. Variability in adequacy is also influenced by dietary patterns; evidence from plant-based populations shows that gaps in vitamin B12, iron, calcium, and DHA required tailored supplementation strategies, underscoring the need to align formulations with dietary context (25).
The absence of choline in all evaluated formulations is particularly concerning given its role in fetal brain development and recent recommendations supporting its inclusion in prenatal nutrition (10,34). This finding is consistent with evidence from diverse populations, where deficiencies in choline, vitamin D, and omega-3 fatty acids persists despite supplement use, while other nutrients may exceed recommended levels (35). These results align with recent expert consensus indicating that current prenatal supplementation practices often fail to reflect updated evidence and recommending a shift from traditional iron-folic acid approaches toward more comprehensive, context specific multiple micronutrient strategies across the life course (36).
In addition, substantial heterogeneity in supplement formulations across countries limits comparability and standardization. Differences in regulatory frameworks, market availability, and prescription practices contributed to variability in nutrient composition, complicating cross-country comparisons and the development of unified supplementation strategies.
Socioeconomic disparities further influence access to and use of supplements, potentially exacerbating nutritional inequalities. Evidence indicates that supplement use is higher among urban and higher-income populations, leaving more vulnerable groups underserved (27,32).
Emerging global recommendations emphasize the importance of preconception nutrition, recognizing that maternal status prior to pregnancy plays a critical role in fetal development and long-term health outcomes (37). Accordingly, expert consensus supports extending micronutrient interventions beyond pregnancy to include the preconception period, given that many women enter pregnancy with existing nutrient deficiencies (36). Current guidelines also support multiple micronutrient supplementation (MMS) to improve birth outcomes, although implementation remains limited in many regions (14,38).
Addressing these gaps requires coordinated public health strategies integrating dietary improvement, fortification, and evidence-based supplementation. While dietary diversification remains fundamental, it is unlikely to resolve widespread deficiencies in the short term (11). Given the intergenerational impact of maternal nutrition, interventions across the preconception, pregnancy, and lactation periods are critical to optimize health trajectories (5). These strategies must balance adequacy and safety, ensuring that supplementation addresses deficiencies without promoting excessive intake, while evolving evidence underscores the need to periodically update nutritional guidelines to reflect current scientific knowledge (39).
Limitations
This study has several limitations. The supplementation analysis represents a theoretical population-level scenario based on mean dietary intake combined with the nutrient composition of a single representative prenatal supplement per country, assuming 100% adherence, which may overestimate real-world intake. Additionally, the contribution of fortified foods was not assessed separately across population subgroups, which influence total nutrient intake.
Dietary data were obtained through self-reported 24-hour recalls and are subject to recall bias, misreporting, and measurement error despite the use of standardized methods. The ELANS sample includes only urban populations, limiting generalizability to rural settings. Nutrient estimates did not account for bioavailability or nutrient–nutrient interactions.
Comparisons between countries are constrained by variability in supplement formulations and selection criteria. Furthermore, analyses were not stratified by dietary diversity or age subgroups. Finally, findings are based on non-pregnant women and therefore reflect preconception conditions rather than actual intake during pregnancy.
Strengths
This study has several strengths. Dietary intake in the ELANS study was assessed using two non-consecutive 24-hour recalls, reducing measurement error and improving the estimation of usual intake. The large, representative sample across multiple countries enhances the generalizability of the findings with urban populations of the region. In addition, this study provides an innovative framework to evaluate prenatal supplementation practices and offers a novel approach to inform strategies for improving micronutrient adequacy among WCA in Latin America.
Conclusions
Significant micronutrient deficiencies persist among WCA in the ELANS study, while prenatal supplementation improves some nutrient intakes but leaves key gaps, particularly for calcium, vitamin E, and choline. At the same time, supplementation frequently leads to excessive intake of nutrients such as iron, vitamin A, and B-complex vitamins. These findings highlight a mismatch between supplement composition and population needs, underscoring the need for tailored, evidence-based strategies to optimize maternal nutrition.
Acknowledgments
The authors would like to thank the staff and participants from each of the participating sites who made substantial contributions to the ELANS.
Conflict of Interest
This article was writing using funds from an Abbott Nutrition Research Grant. The sponsors had no role in the design, data processing and interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Authors' contributions
- MHC, MCYG, LYCS, AR developed and conceptualized the idea and methods.
- PHR, DAY was in charge of the data processing,
- YK, MF, RP, GGS revised and gave input to the manuscript.
- MW, JL revised the manuscript and edit.
References
- Miketinas D, Luo H, Firth JA, Bailey A, Bender T, Gross G, et al. Macronutrient and Micronutrient Intake Among US Women Aged 20 to 44 Years. JAMA Netw Open 2024;7:e2438460. https://doi.org/10.1001/jamanetworkopen.2024.38460.
- Domínguez L, Fernández-Ruiz V, Cámara M. Micronutrients in Food Supplements for Pregnant Women: European Health Claims Assessment. Nutrients 2023;15:4592. https://doi.org/10.3390/nu15214592.
- Hutchesson MJ, de Jonge Mulock Houwer M, Brown HM, Lim S, Moran LJ, Vincze L, et al. Supporting women of childbearing age in the prevention and treatment of overweight and obesity: a scoping review of randomized control trials of behavioral interventions. BMC Womens Health 2020;20:14. https://doi.org/10.1186/s12905-020-0882-3.
- McGowan L, Lennon-Caughey E, Chun C, McKinley MC, Woodside J V. Exploring preconception health beliefs amongst adults of childbearing age in the UK: a qualitative analysis. BMC Pregnancy Childbirth 2020;20:41. https://doi.org/10.1186/s12884-020-2733-5.
- Marshall NE, Abrams B, Barbour LA, Catalano P, Christian P, Friedman JE, et al. The importance of nutrition in pregnancy and lactation: lifelong consequences. Am J Obstet Gynecol 2022;226:607–32. https://doi.org/10.1016/j.ajog.2021.12.035.
- Gomes F, Askari S, Black RE, Christian P, Dewey KG, Mwangi MN, et al. Antenatal multiple micronutrient supplements versus iron‐folic acid supplements and birth outcomes: Analysis by gestational age assessment method. Matern Child Nutr 2023;19. https://doi.org/10.1111/mcn.13509.
- Gómez G, Nogueira Previdelli Á, Fisberg RM, Kovalskys I, Fisberg M, Herrera-Cuenca M, et al. Dietary Diversity and Micronutrients Adequacy in Women of Childbearing Age: Results from ELANS Study. Nutrients 2020;12:1994. https://doi.org/10.3390/nu12071994.
- PAHO (Pan American Health Organization). Anemia in women of reproductive age, and children under-five years in the Region of the Americas. 2022. https://www.paho.org/en/enlace/anemia-women-and-children.
- da Silveira EA, Moura L de AN e, Castro MCR, Kac G, Hadler MCCM, Noll PRES, et al. Prevalence of Vitamin D and Calcium Deficiency and Insufficiency in Women of Childbearing Age and Associated Risk Factors: A Systematic Review and Meta-Analysis. Nutrients 2022;14:4351. https://doi.org/10.3390/nu14204351.
- Herrera-Cuenca M, Yépez García MC, Cortés Sanabria LY, Hernández P, Ramírez G, Vásquez M, et al. Inadequate Intake of Choline and Essential Fatty Acids in Latin American Childbearing-Age Women as a Regional Pre-Conceptional Disadvantage: ELANS Results. Nutrients 2024;16:3150. https://doi.org/10.3390/nu16183150.
- Islam MdH, Nayan MdM, Jubayer A, Amin MdR. A review of the dietary diversity and micronutrient adequacy among the women of reproductive age in low‐ and middleincome countries. Food Sci Nutr 2024;12:1367–79. https://doi.org/10.1002/fsn3.3855.
- UNICEF. Undernourished and Overlooked A global nutrition crisis in adolescent girls and women. 2023. https://www.unicef.org/reports/undernourished-overlooked-nutritioncrisis.
- FAO and FHI 360. Minimum Dietary Diversity for Women: A Guide for Measurement. Rome: 2016.
- Keats EC, Haider BA, Tam E, Bhutta ZA. Multiplemicronutrient supplementation for women during pregnancy. Cochrane Database of Systematic Reviews 2019. https://doi.org/10.1002/14651858.CD004905.pub6.
- Parisi F, di Bartolo I, Savasi V, Cetin I. Micronutrient supplementation in pregnancy: Who, what and how much? Obstet Med 2019;12:5–13. https://doi.org/10.1177/1753495X18769213.
- Castillo-Lancellotti C, Tur JA, Uauy R. Impact of folic acid fortification of flour on neural tube defects: a systematic review. Public Health Nutr 2013;16:901–11. https://doi.org/10.1017/S1368980012003576.
- WHO. WHO recommendations on antenatal care for a positive pregnancy experience. World Health Organization; 2016.
- Yu Y, Feng C, Bédard B, Fraser W, Dubois L. Diet quality during pregnancy and its association with social factors: 3D Cohort Study (Design, Develop, Discover). Matern Child Nutr 2022;18. https://doi.org/10.1111/mcn.13403.
- Kovalskys I, Fisberg M, Gómez G, Rigotti A, Cortés L, Yépez M, et al. Standardization of the Food Composition Database Used in the Latin American Nutrition and Health Study (ELANS). Nutrients 2015;7:7914–24. https://doi.org/10.3390/nu7095373.
- FAO; IFAD; PAHO; UNICEF; WFP; Latin America and the Caribbean - Regional Overview of Food Security and Nutrition 2023. FAO; IFAD; UNICEF; WFP; PAHO; 2023. https://doi.org/10.4060/cc8514en.
- DeSalvo K, Stamm CA, Borgelt LM. Evaluation of reported contents in prescription and over-the-counter prenatal multivitamins. J American Pharmacists Association 2018; 58:258-267.e3. https://doi.org/10.1016/j.japh.2018.02.006.
- Fisberg M, Kovalskys I, Gómez G, Rigotti A, Cortés LY, Herrera-Cuenca M, et al. Latin American Study of Nutrition and Health (ELANS): rationale and study design. BMC Public Health 2015;16:93. https://doi.org/10.1186/s12889-016-2765-y.
- Institute for Health Metrics and Evaluation (IHME). Global Burden of Disease 2023: Findings from the GBD 2023 Study. Seattle, WA: IHME; 2025.
- Azupogo F, Arnold CD, Bliznashka L, Makori N, Njau CN, Malindisa E, et al. Dietary Intake and Nutrient Adequacies among Women of Reproductive Age in Northern Tanzania: A Cross-Sectional Study. J Nutr 2026;156:101238. https://doi.org/10.1016/j.tjnut.2025.11.008.
- Herrero Jiménez MP, del Pozo de la Calle S, Cuadrado Vives C, Escobar Sáez D. Nutritional supplementation in pregnant, lactating women and young children following a plant-based diet: A narrative review of the evidence. Nutrition 2025;136:112778. https://doi.org/10.1016/j.nut.2025.112778.
- Centeno Tablante E, Pachón H, Guetterman HM, Finkelstein JL. Fortification of wheat and maize flour with folic acid for population health outcomes. Cochrane Database of Systematic Reviews 2019;2019. https://doi.org/10.1002/14651858.CD012150.pub2.
- Ba DM, Ssentongo P, Kjerulff KH, Na M, Liu G, Gao X, et al. Adherence to Iron Supplementation in 22 Sub-Saharan African Countries and Associated Factors among Pregnant Women: A Large Population-Based Study. Curr Dev Nutr 2019;3:nzz120. https://doi.org/10.1093/cdn/nzz120.
- WHO. Guideline. Optimal serum and red blood cell folate concentrations in women of reproductive age for prevention of neural tube defects. World Health Organization; 2015.
- Yeneabat T, Adugna H, Asmamaw T, Wubetu M, Admas M, Hailu G, et al. Maternal dietary diversity and micronutrient adequacy during pregnancy and related factors in East Gojjam Zone, Northwest Ethiopia, 2016. BMC Pregnancy Childbirth 2019;19:173. https://doi.org/10.1186/s12884-019-2299-2.
- WHO. Accelerating Anemia Reduction: A Comprehensive Framework for Action. Geneva: World Health Organization; 2023.
- WHO. WHO global anaemia estimates: key findings, 2025. vol. 16. 2025.
- Stevens GA, Beal T, Mbuya MNN, Luo H, Neufeld LM, Addo OY, et al. Micronutrient deficiencies among preschool-aged children and women of reproductive age worldwide: a pooled analysis of individual-level data from populationrepresentative surveys. Lancet Glob Health 2022;10:e1590–9. https://doi.org/10.1016/S2214-109X(22)00367-9.
- Ali SA, Razzaq S, Aziz S, Allana A, Ali AA, Naeem S, et al. Role of iron in the reduction of anemia among women of reproductive age in low-middle income countries: insights from systematic review and meta-analysis. BMC Womens Health 2023;23:184. https://doi.org/10.1186/s12905-023-02291-6.
- Gallo M, Gámiz F. Choline: An Essential Nutrient for Human Health. Nutrients 2023;15:2900. https://doi.org/10.3390/nu15132900.
- Crawford SA, Brown AR, Teruel Camargo J, Kerling EH, Carlson SE, Gajewski BJ, et al. Micronutrient Gaps and Supplement Use in a Diverse Cohort of Pregnant Women. Nutrients 2023;15:3228. https://doi.org/10.3390/nu15143228.
- Cetin I, Devlieger R, Isolauri E, Obeid R, Parisi F, Pilz S, et al. International expert consensus on micronutrient supplement use during the early life course. BMC Pregnancy Childbirth 2025;25:44. https://doi.org/10.1186/s12884-024-07123-5.
- WHO. Preconception care: Maximizing the gains for maternal and child health 2021. https://www.who.int/maternal_child_adolescent/en.
- Smith ER, Shankar AH, Wu LS-F, Aboud S, Adu-Afarwuah S, Ali H, et al. Modifiers of the effect of maternal multiple micronutrient supplementation on stillbirth, birth outcomes, and infant mortality: a meta-analysis of individual patient data from 17 randomized trials in lowincome and middle-income countries. Lancet Glob Health 2017;5: e1090–100. https://doi.org/10.1016/S2214-109X(17)30371-6.
- Mejia-Montilla J, Reyna-Villasmil N, Reyna-Villasmil E. Consumo de micronutrientes durante el embarazo y la lactancia. Rev Peru Ginecol Obstet 2021;67. https://doi.org/10.31403/rpgo.v67i2368.
