
We determined the effect of calcium supplementation on bone mineral density (BMD) and bone mineral content (BMC) and identified predictors of bone mass changes in adolescent mothers 6 months postpartum. A prospective, analytical, clinical study was performed in adolescent mothers (≤19 years old; n=37) from La Plata, Argentina. At 15 days postpartum, mothers were randomly assigned into one of two groups and started with calcium supplementation; one group received dairy products (932 mg Ca; n=19) and the other calcium citrate tablets (1000 mg calcium/day; n=18). Weight, height and dietary intake were measured and BMD was determined by DEXA at 15 days (baseline) and 6 months postpartum. BMC, total body BMD and BMD were assessed in lumbar spine, femoral neck, trochanter and total hip. Regression models were used to identify the relationship of total body BMD and BMC with independent variables (calcium supplementation, months of lactation, weight at 6 months, percent weight change, lean mass at 6 months, percent lean mass change, total calcium intake). Results showed that changes in BMD and BMC at the different sites were similar in both groups, and changes in percent body weight and total calcium intake were the main predictive factors. In conclusion, the effect of calcium was similar with either form of supplementation, i.e., dairy products or tablets, and changes in percent body weight and total calcium intake were predictors of total body BMD and BMC changes.
Key words: Calcium supplementation, bone mineral density, bone mineral content, adolescent mothers, body composition, calcium citrate, dairy product.
El objetivo del estudio fue determinar el efecto de dos formas de suplementare calcio sobre la densidad mineral ósea (DMO) y el contenido mineral óseo (CMO), e identificar predictores de cambios en la masa ósea en madres adolescentes a los 6 meses postparto. Se realizó un estudio prospectivo, analítico y clínico en madres adolescentes (≤19 años; n=37) de la ciudad de La Plata, Argentina. A partir de los 15 días postparto, las adolescentes fueron distribuidas al azar en 2 grupos y comenzaron con la suplementación con calcio; un grupo recibió productos lácteos (932 mg Ca; n=19) y el otro citrato de calcio (1000 mg calcio/día; n=18). Se midió peso, altura y consumo de alimentos y se determinó la DMO por DEXA a los 15 días (línea de base) y a los 6 meses postparto. También se determinó CMO, DMO corporal total y DMO de columna lumbar, cuello femoral, trocánter y cadera total. Se usaron modelos de regresión para identificar relaciones entre DMO corporal total y CMO con variables independientes (tipo de suplementación, meses de lactancia, peso a los 6 meses, porcentaje de cambio de peso, masa magra a los 6 meses, porcentaje de cambio de masa magra, consumo total de calcio). Los resultados muestran que los cambios en DMO y CMO en los distintos sitios fueron similares en ambos grupos, y que los cambios en los porcentajes de peso corporal e ingesta total de calcio fueron los principales factores predictivos. En conclusión, el efecto del calcio fue similar tanto con productos lácteos como con comprimidos. Los cambios porcentuales en peso corporal e ingesta total de calcio resultaron factores predictivos de los cambios de la DMO corporal total y el CMO.
Palabras clave: Suplementación con calcio, densidad mineral ósea, contenido mineral óseo, madres adolescentes, composición corporal, citrato de calcio, productos lácteos.
IDIP – Instituto de Desarrollo e Investigaciones Pediátricas “Prof. D. Fernando E. Viteri”, Hospital de Niños de La Plata, (MS/CIC-PBA), La Plata,Argentina
Bone mass loss and recovery after weaning and resumption of menses have been reported in both lactating adult (1-6) and adolescent (7,8) mothers. In an earlier report of adolescent mothers, we found a significant bone mineral density (BMD) loss at the hip (5%) and in total body BMD (2%), with subsequent bone mass recovery during the 12-month follow-up (8). Such recovery occurred during the early postpartum period and was not related to eventual BMD losses during pregnancy, being slightly lower in younger mothers and in those who had not resumed menses.
Calcium supplementation during lactation has been studied in lactating adult (9,10) and adolescent (11) mothers. In adult women, calcium salts did not have a marked effect; Prentice et al. (9) suggest that breastfeeding women with low calcium intake may not benefit from calcium supplementation, and that the physiological mechanisms developed during lactation provide the necessary calcium for milk production. In the case of Kalwarf et al. (10), the authors found that supplementation with 1 g calcium per day does not prevent bone mass loss during lactation, observing a light improvement in bone mass gain after weaning. On the other hand, Chan et al. (11) have suggested that an adequate calcium intake (dairy products and calcium rich food) may prevent bone loss during lactation in adolescent mothers, and Abrams (12), in an editorial reviewing the effects of calcium supplementation, concludes that adult breastfeeding women would not benefit from a higher calcium intake, but emphasizes the importance of the nutrient in the reproductive cycle. The mentioned author further reports that adolescent breastfeeding mothers are a very important risk group that could benefit from such supplement. In this regard, the percentage of births to women under 20 years of age in Argentina amounts to 15.6% (13), and the National Nutrition and Health Survey (14) indicates that calcium intake in women under the age of 19 is very low (482 mg/day) in our population. In fact, two previous studies performed by our group show that calcium intake in lactating adolescent mothers was <600 mg/day (895 mg/day during puerperium, falling to 547 mg/day 12 months postpartum) (8,15). Other results suggest that low-calcium diets over a prolonged time may impact negatively on one of the critical periods of bone accretion (16).
In view of the above mentioned evidence, the present study aimed to determine the effect of two forms of calcium supplementation on BMD and bone mineral content (BMC), and to identify predictive factors of bone mass change in adolescent mothers 6 months postpartum.
analytical, prospective clinical design was used to assess 37 Caucasian adolescent mothers recruited within 15 days after delivery at the Maternity from the Hospital General de Agudos "José de San Martín", La Plata, Argentina. The city of La Plata is located at 34° South latitude.
Follow-ups were performed at the Outpatient Ward of IDIP – Instituto de Desarrollo e Investigaciones Pediátricas “Prof. Dr Fernando Viteri”, Children´s Hospital “Sor Maria Ludovica”, La Plata, Argentina.
Women who were healthy, ≤ 19 years, primiparous, with term, singleton pregnancy (newborn birth weight ≥ 2500 g) and under natural or intrauterine dispositive (IUD) contraceptive methods were included in the study. Exclusion criteria were mothers who did not breastfeed exclusively for at least 3 months, the presence of chronic and/or acute diseases, history of rickets and osteomalacia, infectious disease the moment of the study, use of any drug, and unwillingness to participate in the study.
A social worker surveyed adolescent mothers within 15 days after delivery, and invited those who complied with the inclusion criteria to participate in the study. Written informed consent was obtained from each adolescent and a responsible adult. A general clinical examination was done before starting the trial; studies and follow-ups were performed at 15 days (baseline) and 6 months postpartum, respectively. A questionnaire about breastfeeding, resumption of menses and contraceptive methods was also performed by the nutritionist and the clinician.
Adolescents were assigned into one of two groups following a systematic random technique. Group 1 (n=19) was given a biscuit fortified with skimmed milk powder (SanCor®, SanCor CUL, Argentina) and the following ingredients: eggs, wheat flour, sugar and vanilla essence. Port salut cheese (SanCor®) (1/2 kg/week) was also given to complete the supplement. This food provided 2073.28 kJ or 496 kcal, 61.2 g carbohydrates, 34.7 g proteins, 11.4 g fat, 932 mg calcium and 0.32 μg vitamin D. The nutritionist asked adolescents to replace some habitual food in their breakfast or snack to avoid a higher calorie intake. They were also asked not to take mineral or vitamin supplements unless they were provided by the healthcare team. Mothers from this group were surveyed weekly when they collected their food and were all given a calendar to record the monthly intake of fortified biscuits and cheese, marking on each day with a cross whether the biscuit or cheese was consumed; the supplement not ingested was subtracted from the daily average intake.
Group 2 (n=18) received 3 capsules of calcium citrate (Calcimax® and Calcimax Forte®, Laboratorios Gador, Buenos Aires, Argentina) providing 1000 mg calcium/day. The assigned supplement was given when participants entered the study (15 days postpartum; baseline) up to 6 months postpartum. Data about calcium supplement intake were collected from telephone follow-ups and pill count. Participants received monthly a bottle of pills with the total number of pills they had to take; on the day of follow-up, pills were counted and the remaining ones, if any, were discounted from the daily average intake.
Body weight was electronically measured with a Tanita 1582 digital balance (100 g accuracy) and height was measured with a SECA 222 stadiometer (mm graduation, 1 cm accuracy) at 15 days and 6 months postpartum. Maximum weight during pregnancy was taken from case histories.
The infant´s feeding pattern was determined by asking mothers whether they were exclusively breastfeeding, bottle feeding, or both. The food-frequency semi-quantitative method was used to estimate the dietary intake of mothers at baseline (15 days postpartum; it reflects the dietary intake during the last months of pregnancy) and 6 months after the study. The survey included calcium dietary intake plus calcium from each dietary supplements (17). All food groups were included in the survey (dairy products, meat, eggs, fruits, vegetables, cereals, beans, flour and derivatives, drinks, candies, fat, oil, and bread). According to the food ingested, the amount of nutrient consumption per day was calculated, estimating daily intake of energy (kJ/day, kcal/day), proteins (g/day), calcium (mg/day), phosphorus (mg/day), and vitamin D (μg/day) with the USDA Food composition data base (18). The questionnaire was designed by a registered nutritionist based on food models to clearly identify serving sizes.
Bone mineral densitometry was assessed by dualenergy-X-ray absorptiometry (DEXA) with a LUNAR DPX-L instrument with pediatric software version 4.6f (GE Lunar Corporation, Madison, WI, USA). The in vivo reproducibility, expressed as percent BMD coeficient of variation, was as follows: lumbar spine (L2-L4), 1.3%; femoral neck (FN), 1.5%; trochanter (TR), 1.4%; total hip (TH), 0.9%; total body BMD, 0.8%. Measurements were performed by a single expert observer. We determined BMC and total body BMD. BMD was measured in all sites and body composition was also estimated by DEXA (19,20). Results were expressed as absolute values (g/cm2), as percent BMD changes in all sites studied, and as percent BMC changes from baseline up to 6 months (final BMD/baseline BMD x 100 [percent BMD] and final BMC/baseline BMC x 100 [percent BMC]). In order to detect a mean 3% difference in BMC variation (β = 0.2; α = 0.05), at least 18 patients per group were needed.
Vitamin D supplement was not recommended because geographical location (latitude 34º) and environmental conditions did not advice about its prescription (21, 22).
The study began at the end of winter-start of spring and follow-ups were made in summer-start of autumn. The study protocol was approved by the Institutional Research Protocols Review Board of IDIP.
The statistical analysis was performed with SPSS version 13 (SPSS Inc, Chicago, IL, USA). Comparisons of means between groups were made with Student ´s t-test for independent samples. Regression models were built to study the relationship of percent BMD and BMC changes (dependent variables) with supplementation group 1 or 2 (dichotomic variable) and months of lactation, weight at 6 months (kg), weight at 6 months (kg)/weight at baseline (kg) x 100, lean mass at 6 months (kg), lean mass at 6 month (kg)/lean mass at baseline (kg) x 100, and total calcium intake (independents variables). The choice of variables was made with backward elimination procedures to obtain the simplest models.
From a total of 37 adolescent mothers, 19 belonged to group 1 (diet supplemented with dairy products) and 18 to group 2 (supplemented with calcium tablets).
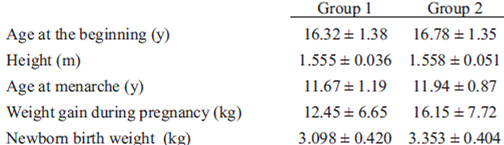
The characteristics of the study sample are depicted in Table 1. The parameters studied did not differ significantly between groups at the beginning of the study. All mothers were exclusively breastfeeding up to 3 months. At 6 months, 15 adolescents in each group continued breastfeeding, while the rest fed their babies with a mixture of bottle feeding and breast milk.
Weight, body mass index (BMI) and percent body fat data (mean and SD) at baseline and 6 months postpartum are presented in Table 2. The analysis of data revealed no significant differences between groups.
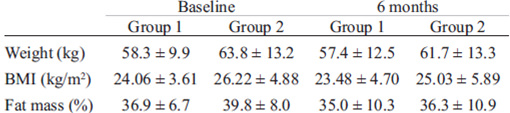
Table 3 shows results of the dietary intake survey, namely, energy (kJ/day, Kcal/day), protein (g/day), calcium (mg/day), phosphorus (mg/day) and vitamin D (μg/day) intake in both groups at baseline and 6 months postpartum. Energy as well as protein intake were higher in Group 1 (p = 0.013 and =0.001, respectively). However, both groups complied with recommendations (22-24).
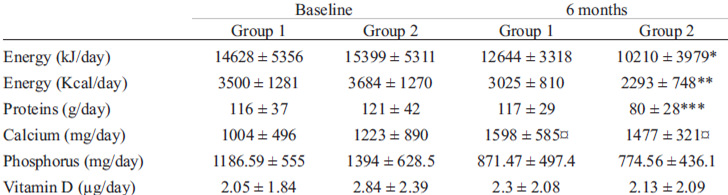
Treatment adherence of adolescent mothers was good (60%); calcium intake (average of the 180 days of intervention) of either form of supplement (dairy products or tablets) was 864 and 839 mg/day in Group 1 and 2, respectively.
Bone densitometry results (absolute value g/cm2) and percent changes from baseline to follow-up are depicted in Table 4. BMD in L2-L4 did not decrease 6 months postpartum in either group.
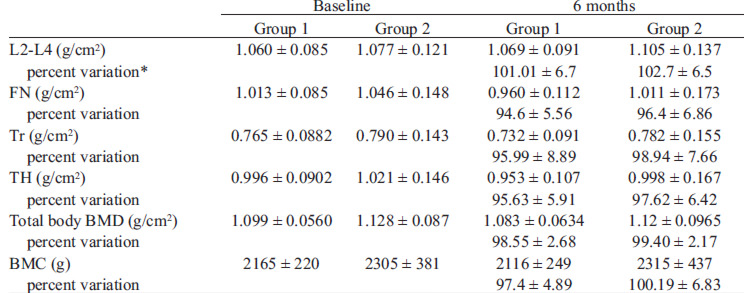
Total body BMD, BMD changes at the different sites (TH, FN and TR) and BMC did not differ between groups.
Regression models for percent changes in total body BMD and percent changes in BMC showed that only percent body weight changes and total calcium intake were significant, and would account for the 38% total body BMD and the 40% BMC variance (Table 5).

To our knowledge, this study is the first to compare two calcium supplements and their effect on BMD at different sites and on BMC in adolescent mothers exclusively breastfeeding for at least 3 months and followed-up during the first 6 months postpartum. Our data suggest that changes in BMD and BMC 6 months postpartum were similar in both intervention groups, and that percent body weight changes and total calcium intake were significant predictors of bone mass change.
Very few reports in the literature have investigated the impact of calcium supplements in the diet or calcium salts on BMD in lactating adolescent mothers. Chan et al. (11) studied the efficacy of a high calcium diet composed of dairy products on BMD loss in lactating adolescent mothers during 4 months. The authors determined BMC by photon absorptiometry of the distal radius, suggesting that bone loss during lactation may be prevented with adequate dietary calcium intakes (>1600 mg Ca/day). However, the current calcium recommendation is lower (1100 mg/day) (24). In our study, supplementation lasted longer (6 month), BMD measurements were performed with another method (densitometry) and in other sites (lumbar spine, total hip, total body), the calcium intake was lower, and two forms of calcium supplementation were compared
The average dietary intake of calcium at baseline in the current study was slightly higher than that reported in our previous report without supplementation (approximately 1000-1200 mg Ca/day vs 895 mg Ca/day) (8). At 6 months postpartum, there was a marked decrease in calcium intake in both the previous and the present report. Apparently, during pregnancy mothers consume more energy, calcium and other nutrients, but do not receive adequate counseling during lactation, when dietary habits are similar to those of the general adolescent population.
The current results show that BMD and BMC of adolescents receiving a calcium supplement in their diet or tablets were similar after the 6-month intervention. Total body BMD and BMC had not significant changes in either study group, and results were similar at different hip sites (FN, TR, TH). Whereas some authors (10,11,25) have studied calcium supplementation in adult and adolescent mothers without evaluating BMD at all hip sites, others (10,25) have measured it in forearm and L2-L4, reporting that calcium supplementation does not prevent bone loss during lactation in L2-L4. In our study, BMD in L2-L4 remained unchanged as compared to that observed at baseline. Similar results were also reported in young adult undernourished women from India without supplementation, who did not present significant BMD losses in L2-L4 6 months postpartum (26).
Chan et al. (11) found correlation between percent BMC changes and calcium intake in lactating adolescent mothers. Our results show that not only percent BMC but also percent total body BMD changes had a linear dependence on calcium intake during the 6-month follow-up.
Concerning changes in anthropometric variables during the 6-month follow-up (weight, BMI and fat mass), they were similar to those published in our previous reports (8,15).
Kulkarni et al. (26) have reported that maternal weight and lean mass in young adult undernourished women from India explained major variations in BMD changes at various skeletal sites. Our findings show that weight rather than lean mass had a significant association with percent total body BMD and percent BMC. Other studies also report such association in adult pregnant women (27,28) and breastfeeding adolescents (8). Evidently, body weight and its lean and fat body mass components are three factors that play a role on bone health.
BMD and BMC variations not only depend on hereditary, racial and hormonal factors, but also on the intake of calcium and other nutrients, the practice of physical activity and the reproductive history (29). During the first two decades of life, during pregnancy and lactation, and particularly during adolescence, calcium intake requirements are high. However, our population can hardly meet calcium recommendations during such a critical period. Further, compliance with the calcium- or tablet-supplemented diet was the result of a sustained and persistent intervention by the participating healthcare team.
Other variables such as duration of exclusive maternal breastfeeding and resumption of menses were not evaluated in this study because most adolescents continued breastfeeding until the end of the intervention and none had resumed menses; thus, their effect on BMD changes could not be assessed.
Results of the regression analysis showed that belonging to either supplementation group was not significant. Therefore, covering the recommended dietary intake (1100 mg) is mostly important, regardless of the source of calcium supply. Probably, an adequate and sustained calcium intake could be reached through a mixed intervention and nutritional advice, without exceeding the recommended upper limits (24).
One of the weaknesses of our study is the absence of a control group. However, the lack of intervention would have been ethically controversial, due to our previous study in adolescent mothers without intervention who evinced bone mineral loss (8). Nevertheless, we believe that a controlled trial would be necessary.
Although both study groups were advised to go on their habitual diet and the only advice was to replace bread or biscuits by the calcium fortified biscuit provided by our team, participants from group 1 spontaneously consumed more energy than those from group 2.
In previous studies in adult and adolescent mothers, either calcium salts or a higher calcium intake through dairy products have been used for calcium supplementation (9-11). However, one of our main objectives was to compare the results obtained with both forms of supplementation, expecting better results with dairy product since it has been reported that not only calcium and vitamin D but also proteins favor bone health (30). Nevertheless, our data showed similar results with either form of supplementation.
Our data suggest that there were no significant changes in BMD and BMC 6 months postpartum in none of the intervention groups, but percent body weight changes and total calcium intake were significant predictors of bone mass change.
This study was supported by a grant from Salud Investiga (National Ministry of Health of Argentina). Thanks are due to SanCor CUL and Laboratorios Gador for the provision of calcium supplements. The authors are grateful to the women who volunteered to take part in the study. Thanks are also due to Adriana Di Maggio for manuscript editing.
Recibido: 06-01-2012
Aceptado: 20-04-2012