
The objective of this study was to analyse the psychometric properties of the Spanish version of the Self-Efficacy Consumption of Fruit and Vegetables Scale among the Spanish population. The sample was made up of 506 subjects who were selected through a convenience sample. The original version was translated from English to Spanish and later was translated back into English, by different translators. Upon translating, not only did the translators keep in mind the grammatical and linguistic aspects of the text, but also the cultural aspects. In order to validate the content of the Scales, the adapted and agreed-upon version of the scale was evaluated by a panel of experts, in order to obtain the final version. Data collection took place between March and September 2017.The internal consistency was tested using Chronbach’s alpha. For the analysis of the structural validity, a factor analysis was carried out on the Self-Efficacy Consumption of Fruit and Vegetables Scale-Spanish version. Kaiser-Meyer Olkin and Bartlett’s test of sphericity (0.90) confirmed that the analysis was suitable. A two-factor structure was confirmed, as in the original scale. The value of Chronbach’s α for the total questionnaire was 0.877, which shows a good internal consistency. In the analysis of the reliability test-retest, a correlation value of 0.79 (p<0.05) was found, demonstrating its temporal stability. The Self-Efficacy Consumption of Fruit and Vegetables questionnaire is a reliable tool to measure self-efficacy in the consumption of fruits and vegetables in the Spanish context.
Key words: Fruit, reliability, self-efficacy, validity, vegetables
El objetivo de este estudio fue analizar las propiedades psicométricas de la versión española del cuestionario Self-Efficacy Consumption of Fruit and Vegetables Scale en la población española. La muestra estuvo constituida por 506 sujetos, seleccionados a través de un muestreo por conveniencia. La versión original fue traducida del inglés al español y después fue retro-traducida al inglés, por diferentes traductores. En las traducciones se consideró no solo los aspectos gramaticales y lingüísticos, sino también los culturales. Para la validación del contenido, la versión adaptada y consensuada de la escala fue evaluada por el panel de expertos, obteniéndose la versión definitiva. La recogida de datos tuvo lugar de marzo a septiembre de 2017. La consistencia interna de la escala fue valorada a través del alfa de Cronbach. Para el análisis de la validez estructural se realizó un análisis factorial del Self-Efficacy Consumption of Fruit and Vegetables Scale-Spanish versión. El test de Kaiser-Meyer Olkin (0.90) y el test de esfericidad de Bartlett confirmó que el análisis era apropiado. Se confirmó una estructura de dos factores, igual que en la escala original. El valor de α de Cronbach para el cuestionario total fue de 0.877, lo que demuestra una buena consistencia interna. En el análisis de la fiabilidad test-retest, se obtuvo un nivel de correlación de 0.79 (p<0.05), demostrando su estabilidad temporal. La Self-Efficacy Consumption of Fruit and Vegetables es una herramienta fiable para medir la autoeficacia en el consumo de frutas y verduras en el contexto español.
Palabras clave: Fruta, fiabilidad, autoeficacia, validez, hortalizas.
https://www.doi.org/10.37527/2018.68.4.001
A diet with a high fruit and vegetable content may be beneficial to our health. There are several studies that have addressed the positive effects of fruit and vegetable consumption, associating it with a lower occurrence of cancer (1), heart disease and other chronic diseases such as diabetes and hypertension, as well as being an effective strategy for weight control (2).
Consuming fruit and vegetables has been shown to reduce obesity (2), which makes it an important public health factor (3). In European countries, the percentage of the population that consume the daily recommended amount of fruit and vegetables, five servings a day (or 400 grams), varies considerably (4). In the last few years, obesity figures have increased (5), and it is estimated that 39% of the global adult population is overweight and around 13% are obese (6). In Europe, the trend has increased at the same rate as the global increase, with 50% of Europeans overweight or obese (7). In the last few years, there has been an increase in overweight or obese adults in Spain, with overweight figures at 39.2% and obesity at 18.5% (7). This situation has made obesity a real public health problem in developed countries (8), and its prevention is a fundamental challenge in the 21st century (4). This would suggest that current interventions in place to improve decision-making about consumption of healthy foods are not effective (9). So, increasing fruit and vegetable consumption is a public health objective, as a low consumption has been associated with approximately 2.8% of total deaths (4). Identifying modifiable factors related to the consumption of these foods allows us to develop interventions that change this nutritional behaviour (10).
Several theories regarding changing health-related behaviours demonstrate the importance of environmental and personal factors (11), highlighting positive association between consuming fruit and vegetables and self-efficacy (3). Self-efficacy is individual confidence that one has in their ability to perform a certain behaviour (11). This construct helps predict if changes in conduct will take place in the individual and whether they will be maintained (12), influencing motivation and persistence in the face of obstacles (13), in addition to being a predicting factor for the adherence to healthrelated behaviour (14). Self-efficacy is associated with a higher consumption of fruit and vegetables (15), as well as with weight loss (13). Improving this self-efficacy is fundamental in the development of healthy habits that involve controlling one’s diet (13).
Additionally, self-efficacy is a cognitive factor of the Health Action Process Approach (HAPA), which recognises the vital role it plays in making changes in habits or behaviour (16). This model provides a theoretical framework for the influence of intentional and self-regulatory factors in starting and maintaining a change in health behaviours. This has been frequently applied to changing habits of consumption of fruit and vegetables (17).
Several studies claim that, although interventions to increase fruit and vegetable consumption are put into place, these usually fail if the individual shows low levels of self-efficacy (12). Low self-efficacy makes the individual unable to overcome challenging obstacles that may stand in the way of their healthy habits, such as the temptation to eat unhealthy foods, and as a result, these plans are not accomplished (17), which is why it is important to have knowledge about self-efficacy, in order to design effective interventions to change behaviours (18).
There are different tools that measure fruit and vegetable intake, but none of them evaluate individual self-efficacy in fruit and vegetable intake (19). Among the most widely-used tools, we can find the Behavioural Risk Factor Surveillance System, more specifically, the dimension of fruit and vegetable consumption. Other tools used include direct observation, keeping dietary records or diaries, the 24-hour Reminder method, questionnaires about frequency of consumption of certain foods, and biomarkers (19). These tools have numerous limitations, such as not addressing selfefficacy as it is related to capacity and desire, as well as not considering the availability and the individual intent to consume fruit and vegetables (20).
On the other hand, various instruments have been developed in order to determine self-efficacy in the consumption of fruit and vegetables, but these have not been shown to have enough validity or reliability (21). Only four scales have been analysed for their relevant validity, but the only one that measures self-efficacy of adult individuals, in the consumption of both fruit and vegetables, is the one developed by Ling and Horwath (22).
The Self-Efficacy Consumption of Fruit and Vegetables Scale (F/V scale), developed in China by Ling and Horwath (22), has also been validated in African-American women (19). This scale allows us to monitor and predict changes in eating behaviour related to an increase in consumption of fruit and vegetables (22). Currently, in Spain, there are no instruments available that allow us the measure self-efficacy in fruit and vegetable consumption among the general public.
Having a tool that can evaluate self-efficacy in fruit and vegetable consumption can be useful in treating patients. Health professionals play an important role in the promotion of healthy behaviours and patient education (23). Additionally, having direct contact between health professionals and patients helps facilitate a change in health behaviours. Health professionals must implement appropriate dietary education and develop effective interventions in order to modify patient behaviour, increasing consumption of fruit and vegetables (24).
The aim of this study was to develop a transcultural adaptation and validation of the Spanish version of the Self-Efficacy Consumption of Fruit and Vegetables Scale questionnaire among the Spanish population.
Study Sample: In order to carry out the validation of a scale among the general population, the sample must have similar characteristics to the population of study (25). For this reason, a convenience sample was used. The sample was made up of 506 subjects. Inclusion criteria included: being 18 years of age or older and being a native Spaniard. The exclusion criteria included: having any kind of cognitive impairment that impedes full comprehension of the questionnaire. Considering the recommendations of 5 to 10 subjects per test item test (26), an estimated 120 subjects was calculated to be enough to analyse the psychometric properties of the assessment.
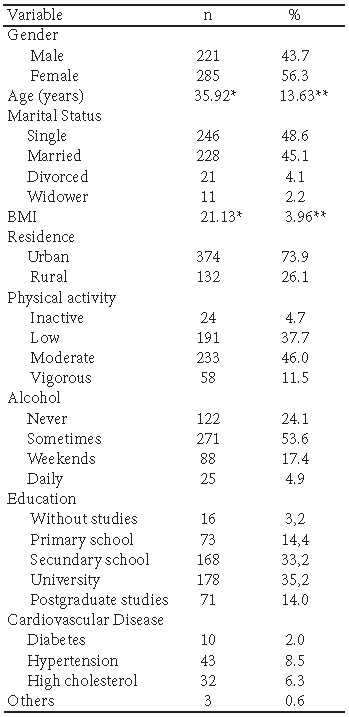
Measure: Firstly, the following sociodemographic variables were collected: sex, age, marital status, education level, place of residence, as well as body mass index (BMI), alcohol consumption, any chronic diseases and level of physical activity.
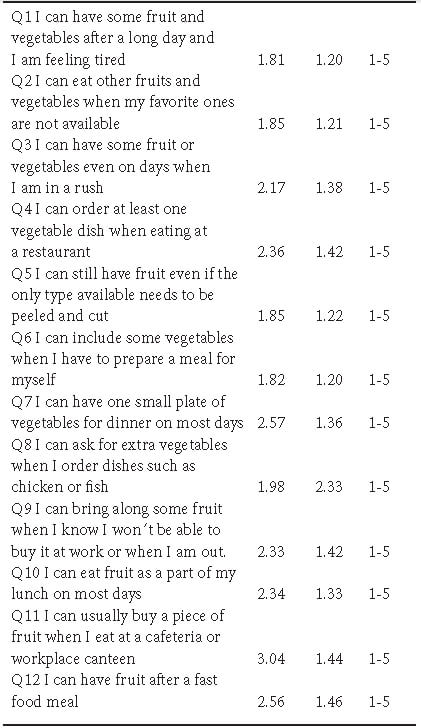
The F/V scale was developed and validated by Ling and Horwath (22). The F/V Scale allows us to evaluate the perceived beliefs of the subjects with regards to the decision to consume fruits and vegetables in different situations. The scale is made up of 12 items, each one rated on a Likerttype scale of 1 to 5, with 1 being totally confident and 5 being not at all confident. The total score is found by adding up the values of each of the items, which may give a range of scores between 12 and 60. Higher scores indicate stronger beliefs about intent to consume fruit and vegetables. The scale is divided into two main dimensions: Remembering to eat (Q1, 3, 4, 6, 11) and Difficult Situations (Q2, 5, 7, 8, 9, 10, 12). The reliability, which verifies the internal consistency of the scale, is quite high, with a total Chronbach value of 0.89, with a minimum accepted value of 0.7.
Procedure: First, the main researcher asked for the corresponding permission from the authors of the original scale, who agreed to its use. The procedure was divided in two phases: (1) transcultural adaptation of the questionnaire and (2) validation of the questionnaire (Figure 1).
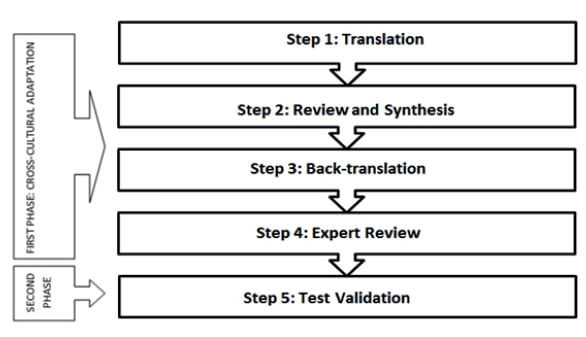
To carry out the cultural adaptation, a protocol of translation-back translation based on the standardised recommendations set forth by Beaton et al. (25). The translation of the F/V Scale from its original language to Spanish was carried out individually by two bilingual native Spanish experts, and two different versions of the scale were obtained. These translators were informed of the objective of the study to minimise individual misinterpretations. The two versions were revised, compared, and each item on the translated scales was analysed in a systematic way. Any confusing terms and concepts were discussed by various members of the research team and the translators, from which we obtained the first version of the scale in Spanish. Subsequently, a pilot study was performed with the version obtained in order to detect cultural and language errors that may have been produced during the translation. For this study, a representative sample of the study population consisting of 60 participants was selected through a convenience sample, obtaining the second version of the scale.
From this second version, a translation was then performed back to the scale’s original language, by two native English translators, individually, who did not know the objective of the study and the original version of the scale. All the versions obtained, including the original version, were systematically revised by a panel of experts, made up of psychologists, psychiatrists, nutritionists and endocrine doctors with more than 10 years of professional experience, who evaluated its comprehensibility, socio-linguistic characteristics and semantic equivalence. Any terms that created discrepancies were debated, until an agreement was reached, however, always keeping the meaning of the question in mind and making sure to not change the meaning of any items that made up the scale. As a result, the final version of the F/V Scale was obtained.
Firstly, the project was approved by the Institutional Review Board of the University. Data collection was carried out in various neighbourhood associations throughout the city of Almeria, on the university campus and at other higher education institutions throughout the city. These places were previously contacted in order to make an appointment and explain the study. The participants were gathered to fill out the questionnaire in a voluntary manner. All the participants were informed about the objective of the research, as well as the anonymity and confidentiality of their data, as well as informing them that they could stop their participation in the study at any time. Those participants that wanted to take part in the study, signed the informed consent form before doing so. Three weeks after the initial questionnaire, a re-test was completed by the same initial sample, in order to evaluate the temporal stability of the responses. Data collection took place between March and September 2017.
In order to validate the content, the adapted and agreed upon F/V scale was evaluated by the panel of experts, and from that, the definitive version was obtained. In regards to the structural validation and the reliability, the relevant analyses were carried out and are described below in the Results section.
Data Analysis: The statistical programme SPSS version 23 was used for data analysis. First, a descriptive statistical analysis was performed on the sociodemographic variables. For the quantitative variables, measures of central tendency and dispersion were calculated (mean and standard deviation), whereas, for the categorical variables, frequencies and percentages were calculated. Construct Validity of the F/V scale was assessed using confirmatory factor analysis (CFA), confirming its suitability using Bartlett’s test of sphericity. In addition, the Kaiser-Meyer-Olkin (KMO) test was used to check the sample suitability. For the correlation between items, Pearson’s correlation coefficient was used. In order to analyse the internal consistency, the value of Chronbach’s alpha was calculated. The testretest reliability was evaluated with Pearson’s correlation coefficient. Statistical significance was set at p<0.05.
Out of the total number of participants (N=506), 43.7% (n=221) were men and 56.3% (n=285) were women. The average age was 35.92 (SD=13.63). Regarding marital status, almost half of the participants were married (45.1%, n=228), and the other half single (48.6%, n=246). The average BMI was 21.13 (SD=3.96). Regarding physical activity, almost half of the sample, 46% (n=233), had moderate physical activity. On the other hand, the majority of the participants did not have cardiovascular disease. The main socio-demographic characteristics of the participants are shown in Table 1.
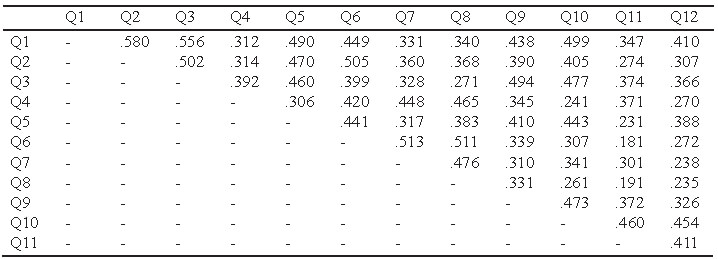
In Table 2, the average scores and standard deviations can be seen for each question of the questionnaire. Table 3 shows the inter-item correlation between the F/V scale questions. All the questions correlated with each other with a value of p<0.01 and a range from 0.181 to 0.580.
To test the validity of the content, the adapted and agreed-upon version of the F/V scale was evaluated by the panel of experts, and from there, a final version was achieved, as described in the Method section. On the other hand, for the analysis of the structural validity of the questionnaire, a factor analysis was performed The KMO test gave a value of 0.90, above the minimum acceptable value of 0.70. Additionally, the factor analysis was found appropriate through Bartlett’s test of sphericity (X2(66) =2242.792; p<0.05).
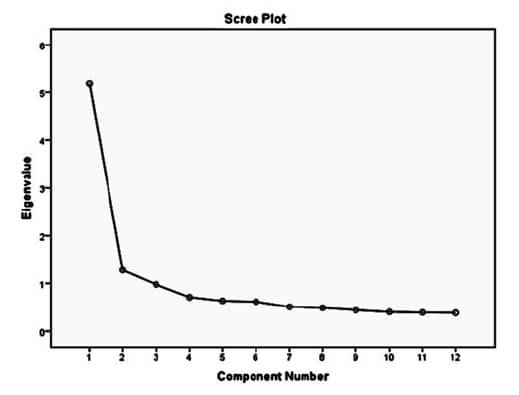
A two-factor structure, as well as the original scale, were confirmed. Another test used to confirm the twofactor structure was the interpretation of the Scree plot graph, where it is observed that from factor II, the values begin to descend below 1 (Fig. 2). Two factors explaining a total of 53.94% of variances were distinguished in the analyses conducted. The first factor explains a 43.30% variance, while the second factor a 10.63% variance.
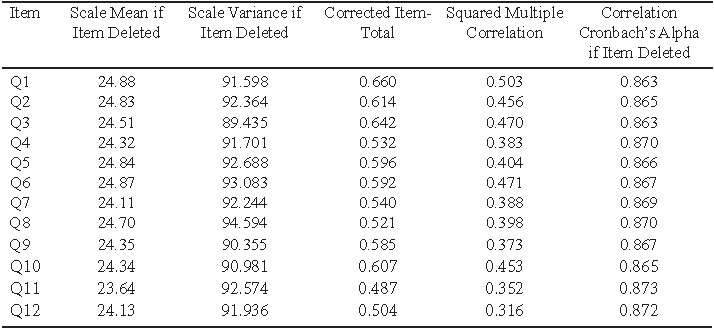
The F/V scale had a Chronbach’s alpha value of 0.877, which indicates good internal consistency. Each one of the items in the scale obtained scores >7, which is the minimum acceptable value, which shows good internal consistency. On the other hand, considering the reliability of each question, Chronbach’s α value was taken into consideration when any of the items were eliminated. All values were found to be in a range between 0.863-0.873, and therefore deleting any of the items was not proved beneficial (Table 4). In the analysis of the test-retest reliability, a correlation level of 0.79 was obtained (p<0.05).
The objective of this study was to develop a transcultural adaptation and validation of the Spanish version of the Self-Efficacy Consumption of Fruit and Vegetables among the Spanish population.
Self-efficacy in fruit and vegetable consumption is associated with various socio-demographic variables, such as age and gender. Various studies report that women usually show higher level of self-efficacy than men, which could be due to the fact that women are more interested in seeking nutritional advice (18, 21). In addition, self-efficacy in fruit and vegetable consumption has been observed to increase with age, which could be related to a change in food preparation habits (21, 22). Another variable to consider is the body mass index; in this study, more than half of the participants were at a healthy weight. This data matched that of previous studies that set overweight and obesity levels in Spain below the European average (27, 28). In addition, regarding physical exercises, the data obtained is similar to that found in other research (29). Regarding cardiovascular diseases, the majority of participants reported not having any; these figures are lower than those reported in other studies, which place the prevalence of heart disease above the average obtained in this study (28, 29).
Regarding the data obtained, after the analysis of the psychometric properties of the transculturally adapted version, and its comparison to the original version, developed by Ling and Howart (22), the twofactor structure was confirmed: “difficult situations” and “being able to remember situations.” However, in the adapted and validated version among African-American women by Gittner and Gittner (19), the two factors merged into one. The 12 items that made up the scale have been maintained in both versions. Regarding the correlation between the items, all the values were found to be at a higher range than those found in the adaptation of the study among African-American women. In relation to the psychometric properties of the scale, a good internal consistency was obtained, with a Chronbach’s α value of 0.877, similar to that obtained by the original authors (22). On the other hand, the structural validity of the questionnaire was high (0.90), above the minimum acceptable level (0.70). As for the temporal stability of the scale, a high reproducibility level (0.79) was found, which was unable to be compared to other studies, as the original authors did not report data on the temporal stability of the assessment. The results obtained demonstrate the reliability and validity of this tool.
Having a tool that allows us to evaluate self-efficacy in fruit and vegetable consumption is important, because self-efficacy has been shown to be an important predictor and indicator in incorporating and modifying healthy behaviours (17). The promotion and access to a healthy diet, with a high fruit and vegetable content, is key to improving and maintaining the health, wellbeing, and quality of life of the population (30). Additionally, Spaniards have considerably modified their diet, decreasing their adherence to the Mediterranean diet (27). Despite this fact, Spaniards still show a higher adherence to the Mediterranean diet than other countries in the Mediterranean region (31). In addition, the Mediterranean diet, based on high consumption of fruits, vegetable, whole grains, pulses and olive oil as the main source of fat, is being replaced by Western food patterns (32). Along these same lines, calorie and nutrient intake in Spain is characterised by a high consumption of proteins, lipids, and a low consumption of carbohydrates, but there has been an increased intake of meat, processed foods and sweets shown (27). As for the consumption of fruit and vegetables, it has also been associated with age, and the young population has been said to consume less than half of the recommended daily amount (33).
On the other hand, other studies carried out in Spain have linked gender to the consumption of fruit and vegetables, with women being the ones who consume the most (28, 29). This may be due to the desire to lose weight (29) or because they tend to have a healthier lifestyle (34). In general, the Spanish population has a low consumption of fruits and vegetables (31).
Therefore, it is important to improve adherence to the Mediterranean Diet, which has been proposed and commonly accepted as a mode of prevention and control of chronic non-communicable diseases (32). Specifically, fruits and vegetables have also been shown to reduce numerous chronic diseases, hence the importance of promoting their consumption (30).
Despite the results obtained, which indicate a strong reliability and validity of the questionnaire, the study data should be contemplated while keeping in mind a set of limitations. The sample was selected by a convenience sample, which affects the generalisation of the results among the general population. The ideal population on which to carry out a validation study would have been a representative sample of adults on a national level, but this type of recruitment has been attempted without success (35). Secondly, the data reported on fruit and vegetable consumption are based on self-reporting, and could be slanted due to recall bias. Future studies should complete the self-reporting with biomarkers, widely used in food behaviour research. The lack of instruments of study which are transculturally adapted and validated to the Spanish context makes it difficult to compare the results with other studies, hence the importance of this study.
The Self-Efficacy Consumption of Fruit and Vegetables Questionnaire has been shown to be a reliable and valid took to measure self-efficacy in fruit and vegetable consumption. Having a tool that allows us to measure self-efficacy in fruit and vegetable consumption is important, because at a clinical level, it has been shown that self-efficacy is an important predictor of incorporating and modifying healthy behaviours. Health professionals, therefore, could have a new tool at their disposal to promote lifestyle changes among their patients, and to acquire healthy habits that allow for the reduction of excess weight and obesity.
Recibido: 06-09-2018
Aceptado: 10-12-2018