
Eating attitudes are defined as beliefs, thoughts, feelings and behaviors towards food. Bulimia nervosa (BN) is an eating disorder, in which the eating attitudes are seriously disturbed. Studies that evaluated nutritional aspects of BN focus mainly on food intake, dietary restriction and binge eating, while the follow-up studies evaluate mainly clinical symptoms. The objective of this study was to evaluate eating attitudes of patients with BN, during and after cognitive-behavioral intervention. Thirty nine (39) BN female patients received cognitive behavioral treatment with a multidisciplinary team and had eating attitudes assessed by a questionnaire developed for this research. Frequencies of the attitudes assessed were compared at baseline, after 12 weeks and 24 weeks of treatment. After treatment, patients had less distorted beliefs about food, less guilty after eating “forbidden” foods and they felt more tranquil while eating outside home. Other negative behaviors, as dietary restriction, the desire of not eat, being angry when feeling hungry and using the food to relive stress, persisted. Eating attitudes of patients with BN are hard to be changed in a short-term. More attention to this disease’s component and new approaches to treatment are needed in order to have a better recovery.
Key words: Eating attitudes, bulimia nervosa, recovery, nutrition therapy.
Atitudes alimentares são definidas como crenças, pensamentos, sentimentos e comportamentos para com os alimentos. Bulimia Nervosa (BN) é um transtorno alimentar no qual as atitudes alimentares estão seriamente perturbadas. Os estudos que avaliam aspectos nutricionais centram sua atenção principalmente na ingestão alimentar, restrição alimentar e compulsão alimentar, e os estudos de seguimento avaliam essencialmente os sintomas clínicos. O objetivo deste estudo foi avaliar as atitudes alimentares de pacientes com BN durante e depois de uma intervenção cognitivo comportamental. Trinta e nove (39) pacientes do sexo feminino receberam tratamento cognitivo comportamental com equipe multidisciplinar e tiveram suas atitudes alimentares avaliadas por um instrumento desenvolvido para esta investigação. A freqüência de diferentes atitudes foi comparada antes, depois de 12 semanas e 24 semanas de tratamento. Depois do tratamento as pacientes apresentaram menos crenças distorcidas sobre alimentação, menos culpa depois de ingerir alimentos “proibidos” e demonstraram mais tranqüilidade para comer fora de casa. Outras atitudes negativas, como restrição alimentar, o desejo de não comer, a raiva de sentir fome e usar o alimento para aliviar questões emocionais persistiram. Conclui-se que as atitudes alimentares de pacientes con BN são difíceis de serem modificadas em curto prazo. Maior atenção a este componente do distúrbio e novas formas de tratamento são necessárias para obter uma recuperação mais completa.
Palavras chave: Atitudes alimentares, bulimia nervosa, recuperação, terapia nutricional.
University of São Paulo / Nutrition Department - Public Health School – University of São Paulo. Brazil
Eating attitudes are defined as beliefs, thoughts, feelings and behaviors towards food (1). The normal eating attitude involves a proper comprehension of the role of food in life: physiological, emotional and social. When eating attitudes are considered, food could not be simply thought in a physiologic manner, and the food choices are not made based merely on their nutritional contribution.
Bulimia nervosa (BN) is an eating disorder (ED) marked by binge eating and compensatory practices, with highly affected eating attitudes, such as misconceptions about nutrition, false beliefs and feelings of hate and incompetence in dealing with food (2-5).
There are no specific data regarding prevalence of ED in Brazil. Case reports from developing countries are rare; thus, it gives the wrong impression that these disorders are rare in non-developed countries (6). Anyhow, it is known that the incidence of ED has been increasing in less developed countries (7). It is estimated that the prevalence of ED in Brazil is similar to that observed in western countries for young women: 0.5% for anorexia nervosa; 1.0% for bulimia nervosa, and 2-5% if partial syndromes are considered (8).
Nutritional therapy plays a relevant role with regards to treatment goals, which should be provided by a specialized dietitian aiming to end bulimic behavior and to change the patient’s attitudes towards food (2,3,9).
To assess the effects of BN treatment, most studies analyze the frequency of bulimic behavior (vomiting episodes, for example) (10). Few studies have assessed the nutritional evolution of bulimic patients (1,11,12,13) and as far as we know just one study had evaluated some measures of eating attitude after treatment (6), therefore, this issue requires further research (14).
We could not find any instrument that measures this construct adequately. Many studies misuse the term eating attitudes, so that the questionnaires that claim to measure eating attitudes, in fact evaluate if some groups of foods are bought and eaten (15,16). Some studies focus on behavior that is unique to eating disorders, but their questions only cover the classical symptoms of BN, like vomiting frequency (17).
There are some widely used scales in ED research (18-21), which, although useful and well-developed, are limited in scope, and measure mainly uncontrolled eating, dietary restraint, and the subjective feeling of hunger, but they do not encompass the full range of dysfunctional eating attitudes that BN implies. Even the Eating Attitude Test (EAT) (21) despite its name, focus especially in restraint and is more useful for screening purposes. It measures some eating attitude such as thinking a lot about food and the feeling that food controls life, but ignores others like relationship with food. In this manner, using these questionnaires provides several relevant information, excluding others, such as beliefs and perceptions about food, pleasure of eating, hidden eating, difficulty in dealing with hunger, social events, food choices, and feelings towards food.
Thus, this article aims to evaluate possible changes in some attitudes, beliefs and feelings during and after treatment in Brazilian bulimic patients. We put forward a hypothesis that the traditional treatment would be able to improve some eating attitude, but most of them are difficult to be modified.
We invited 55 female BN patients that seek for treatment at Eating Disorders Unit - AMBULIM - Brazil to be part of this research; 39 of them fulfilled the inclusion criteria and were admitted for treatment and accepted to participate. The following inclusion criteria were used for this study: being diagnosed with bulimia nervosa according to the DSM-IV criteria (3), as established by a psychiatrist; being female and 17 years of age or older; having had no psychiatric and/or psychological treatment and/or nutritional treatment at the moment of recruitment. The exclusion criteria included: having psychosis; abusing or being addicted to a drug and alcohol; being diagnosed with severe depression; admitted in an inpatient treatment at the moment of recruitment.
The study was a six-month follow up in which eating attitudes were evaluated. Measurements were performed at baseline (Phase 1), after 12 weeks of structured cognitive behavioral therapy - CBT (Phase 2) and after 24 weeks of CBT (Phase 3). Patients underwent a clinical interview that yielded descriptive data (age, weight, height) and had their Body Mass Index (BMI – weigh in kg/height2 in meters) calculated.
The setting for the intervention was an outpatient unit of a public hospital. The treatment consisted of cognitive behavioral therapy with one weekly consultation with a psychiatrist, a psychologist and a dietitian.
Weekly nutritional treatment consisted of one hour of nutrition education in group and 30 minutes of individual counseling based on their food diaries. The following topics were addressed during the education sessions (12 weeks): role of nutrients, energy and nutrient requirements; food pyramid; ineffectiveness of dietary restraint; concepts of hunger and satiety; adequate weight and build; guidelines for buying food and eating at social events. After this structured period, the topics discussed were those that patients and/or the professional team chose and included issues from lay magazines about body and diet, the social and emotional roles of food and strategies to handle difficult situations regarding eating.
The psychiatry treatment was done in individual appointments in a cognitive focus and the medication was prescribed according to the evaluation of the doctor. The psychological therapy was done in group sessions using a cognitive approach in which the following issues were addressed: the kinds of hunger (physical, emotional and social); the beliefs involved in the diet-binge-purge cycle; the personal meaning of BN; body image dysfunctions; mechanisms used in order to copy with the emotions; and barriers for change.
Patients filled in a questionnaire (22 questions) about their eating attitudes and relationship with food specially developed for this research. The questions were derived from our clinical experience (based on the myths and misconceptions that patients usually report) and from other scales that in a certain manner approach eating attitudes in EDs (18-21). The tool had been previously applied in a sample of patients to check if it was clear and easily understandable.
Descriptive data are presented as mean and standard deviation. The software Statistical Package for Social Sciences (SPSS) for Windows V6.0 was used. The level of significance adopted was p < 0.05.
The questions regarding eating attitudes and beliefs were evaluated by frequency of positive or negative responses. For questions about relationship with food patients responded in a Likert Scale, in which the answers were analyzed by putting the first three options (always, very often, often) together as “frequent thought or feeling”, and the last three (sometimes, rarely, never) as “infrequent thought or feeling”. The ratio of positive responses for questions was compared among the phases by means of a chi-square test. The same test was used to compare the ratio of frequent and infrequent answers for the questions of relationship towards food among the phases.
Subjects gave written consent to participate. The protocol of this research was approved by the ethical committee at Public Health School of University of Sao Paulo.
Most patients (90%) presented purging subtype of BN. The duration of the disorder ranged from 1-20 years. The mean age was 28 + 6 years; mean BMI was 23 + 4 kg/m2 and 65% had at least started college.
From 39 patients (age range 21-35) who had initiated the treatment, twenty had finished the 12 weeks of cognitive behavioral therapy, and 15 underwent the entire 24-week follow-up. Dropout rate was 61.54%. Therefore, the responses for baseline correspond to 39 patients, Phase 2 to 20 patients and Phase 3 to 15 patients. The reasons for dropout of treatment were: lack of motivation; difficulty with fixed schedule for treatment (that demand one entire afternoon period during the week); and the occurrence of holydays and vacation period between the follow-up (December and January).
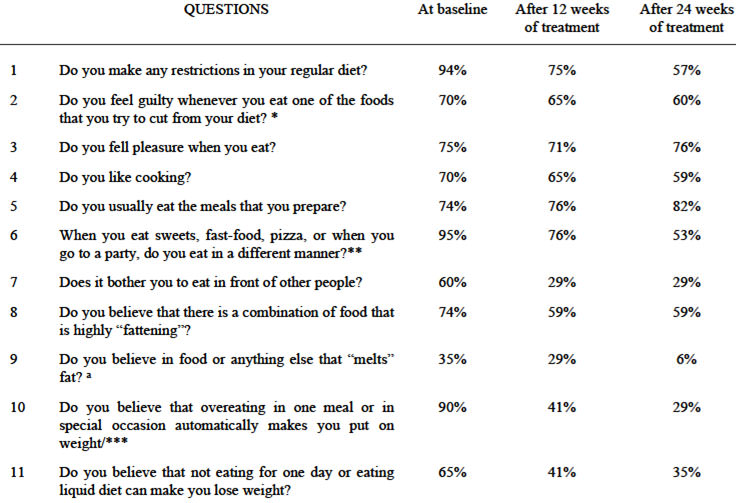
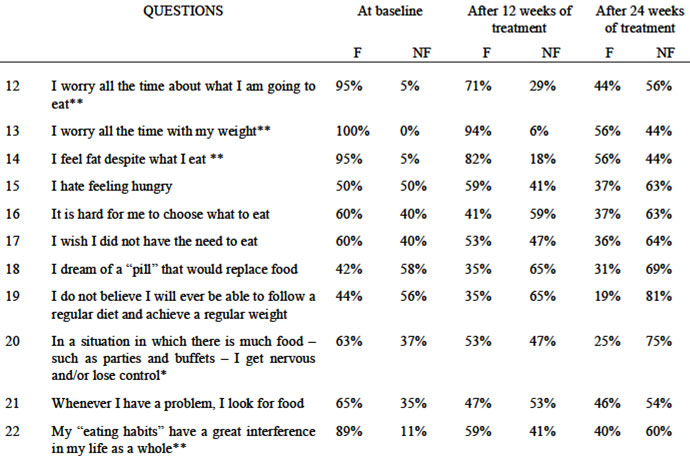
Table 1 shows the frequencies of affirmative responses for questions about eating attitudes and beliefs. Table 2 shows the responses for questions about the relationship with food.
A study carried out with the same sample (1) showed a significant reduction in the frequency of binge and vomiting episodes, and after 24 weeks of treatment, patients no longer met the diagnosis criteria according to the DSM-IV (3). In spite of that, the inappropriate eating attitudes and relationship with food remained.
The reduction of guilt statements when patients ate food whose consumption they had restricted characterizes greater permissiveness towards these foods. There was a gradual decline in statements regarding behavior change after eating sweets, fast food, and “different” food; however, less than half of the patients changed. It is noteworthy that, even with significant changes, most of them were still feeling guilty and having difficulties with “dangerous” food, as mentioned by Keller et al. (22).
More than half of the patients were still imposing some type of restraint at the end of 24 weeks. This confirms that diet restraint is a common symptom in BN and that it is difficult to eliminate (22). No important changes were found in the statements regarding eating with pleasure. We believe that treatment does not change feelings and relationship with food as much as behaviors. Patients seem to associate food preparation with the possibility of loosing control and eventually dislike it, as suggested by the gradual decrease of affirmative answers regarding to the enjoyment of cooking.
Among the beliefs about diet, significant reductions were observed only in the proportion of patients who thought they would put on weight immediately after eating and who believed that something could melt fat (p value was close to significance). Part of them still believed that some combinations were especially “fattening” and that fasting would make them lose weight, which suggests that in spite of all the information received, suspicion in relation to food remained.
At the end of follow-up, most of them no longer worried about food all the time, possibly due to the establishment of a regular diet pattern as the relationship between obsessive dieting and extreme diet concern is a well-known fact (23). There was also a significant reduction concerning feeling fat regardless of what they ate, which could suggest that the treatment succeeded in addressing some body image issues, as recommended (24). However, many patients remained with those perceptions and feelings, which is confirmed by some authors (25-27) that, regardless of the result of the treatment, weight fluctuations and body dissatisfaction persisted.
Regarding the question of feeling nervous or lacking control with abundant food, the most relevant reduction took place at the end of the 24 weeks, indicating that longer treatment is necessary to gain confidence to eat in any situation. The analysis of the question about “the way you eat” interfering greatly in their lives show significant reduction, although 40% still answering frequently at the end, indicating that to a subgroup, BN portrayed the complex role of food in life.
There were no significant changes in the question related to looking for food whenever they have a problem, suggesting that food still played many different roles in these patients ´ lives, as an expression of feelings and also a way to deal with external and internal demands. Thus, faced with a multitude of possibilities, ED patients choose weight and food control, as a way of life. Changing this attitude pattern seems to require longer treatment.
No significant changes were observed in the answers about “being angry when feeling hungry”, “having difficulty in choosing foods”, “the desire of a pill that replaced meals” and “I wish I did not have to eat”. These data illustrate the inadequate relationship with food, denying the physiological and emotional needs for eating (22).
It is stated (28) that longer treatment leads to better results. Our results indicate that 12 weeks of cognitive behavioral therapy are not enough to significantly change eating attitudes, as only a few significant changes were detected. After 24 weeks changes were more consistent. However, follow-up time was short and patients may have suffered relapses after this period.
One should also consider that the nutritional approach of the treatment focused on nutritional education and that there was no specific approach to address the relationship with food. Some authors (29,30) say that traditional cognitive behavioral therapy is not enough to improve body image issues in EDs, and that specific interventions are necessary for that purpose. One can conclude that the same is valid for the eating attitudes and relationship towards food. We believe that one of the main challenges of nutritional therapy is how to change bulimia patient’s dysfunctional attitudes, taking in to account that traditional nutrition education does not modify beliefs and distorted cognitions.
Some remarks must be made about this study; first, it was conducted with a relatively small group of patients, which became even smaller due to the high dropout rate. But BN is characterized by relapses and high dropout rates (31,32). We believe, however, that the number of patients who completed the process was relevant, as there are only a few studies working with nutritional variables and, specifically, with these deeper concepts that are eating attitudes.
Second, the instrument used was developed for this research, and it was not validated; we have to remember anyway that other tools used to evaluate eating attitudes in ED patients (9) or in general population (33) were not validated either. The scale used here was a starting point for the development of a specific tool to measure eating attitudes, and today, based on the results of this study, it is being adapted and tested psychometrically.
We believe it is important to research these aspects of eating attitudes, because even the patients whose clinical status becomes normal may still have a complicated relationship with eating and their bodies. This may, in turn, cause psychological distress and probably lead to relapses.
As we believed, some significant changes in eating attitudes of these BN patients were found after 24 weeks of treatment, but some could not be modified.
The main goal of the traditional nutritional approach for BN is to achieve a normal eating pattern and to eliminate the purging practices but further nutritional treatment, based specially on counseling, should aim to help the patient to enhance changes in eating attitudes.
Dietitians that work with ED should be able to understand and treat all the dysfunctional eating attitudes presented by BN patients and not only the bulimic episodes that define this syndrome, therefore it is important to seek training in counseling, cognitive techniques and motivational interviewing to improve the treatment of all features of patients´ eating attitudes.
We are thankful to Karin Louise Lenz Dunker, PhD, for her help with the data bank. The authors would like to thank The State of Sao Paulo Research Foundation - FAPESP - for the post doctorate scholarship that supports Marle. S Alvarenga (process 06/56850-9) and Fernanda B. Scagliusi (process 07/59141-1).
Recibido: 24-10-2007
Aceptado: 15-08-2008