
Like many other developing countries, Brazil has been going a nutritional transition which presence both malnutrition and overweight. Stunting and overweight are the major public health problems in Brazilian children. The objective of this study was to document the prevalence of stunting, overweight and anemia in preschool children and examine if those nutritional problems are related; also identify if these nutritional problems have the same risk factors. Data from the “Efficient Daycare Center Project” which include 270 children attending nurseries of eight daycare centers in Sao Paulo city, Brazil were used for this study. Data on height and weight were converted to z-scores using WHO anthro software. Hemoglobin (Hb) concentrations were determined on finger-prick blood samples. The co-occurrence of stunting, overweight and anemia was investigated by contingency tables a log-linear model. Univariate and multiple regression analyses were performed to estimate the association of HAZ, WAZ, WHZ and Hb levels with their risk factors. The results showed high prevalence of overweight (22.2%), risk of stunting (22.6%) and anemia (37%). Percent of daycare attendance, age, number of siblings under 5 years old and per capita income are associated with Hb levels. This study provides evidence that Brazil is going through a nutritional transition and suggest that the adoption of public policies to expand and improve services in daycare centers may help to prevent multi-nutritional problems in preschool children.
Key words: Anemia, child, child day care center, nutritional status, risk factors.
Como muchos otros países en desenvolvimiento Brasil esta pasando por la transición nutricional, la cual tiene presente a la desnutrición y sobrepeso. Este estudio tuvo como objetivo mostrar la prevalencia de baja estatura, sobrepeso y anemia en niños en edad preescolar y analizar si esos problemas nutricionales están relacionados; también identificar si esos problemas nutricionales presentan los mismos factores de riesgo. Fueron utilizados datos del “Proyecto CrechEficiente” el cual estudio 270 niños que asisten a cunas de ocho jardines de la infancia en la ciudad de Sao Paulo, Brasil. Los datos de peso y estatura fueron convertidos en z-escore utilizando el software WHO Anthro. La extracción de sangre para la determinación de hemoglobina (Hb) se realizó por punción digital. La co-ocurrencia de baja estatura, sobrepeso y anemia fue investigada a tráves de tablas de contingencia y modelo loglinear. Fueron realizados análisis univariados y regresión múltiple para determinar la asociación entre TEZ, PEZ, PTZ y niveles de hemoglobina con sus factores de riesgo. Los resultados mostraran elevada prevalencia de sobrepeso (22,2%), riesgo para baja estatura (22,6%) y anemia (37%). El porcentaje de frecuencia a los jardines infantiles, edad, número de hermanos menores de 5 años y renta per cápita están asociados con los niveles de hemoglobina. Este estudio muestra evidencia de que el Brasil esta pasando por una transición nutricional y sugiere adopción de políticas públicas para difundir y mejorar los servicios de los jardines infantiles pudiendo ayudar a prevenir varios problemas nutricionales en niños en edad preescolar.
Palabras clave: Anemia, niño, jardines infantiles, estado nutricional, factores de riesgo.
Department of Pediatrics, Universidade Federal de Sao Paulo, Sao Paulo, Brazil, Nutrition and Health Sciences Program, Hubert Department of Global Health, Emory University, Atlanta, GA, USA.
A nutritional transition has been observed in developing countries that are experiencing rapid and intense changes in economic growth and demographic structure. In the past decades, conditions favoring the occurrence of nutritional deficiencies gradually gave way to an epidemic of obesity and chronic diseases related to excessive and unbalanced food consumption and inadequate physical activities (1-4). This pattern affects all populations, particularly children. Globally, childhood malnutrition and nutritional deficiencies reduces while childhood obesity continues to rise (5,6).
Like many other developing countries, Brazil has been going a nutritional transition which presence both malnutrition and overweight. Stunting and overweight are the major public health problems in Brazilian children. Studies conducted in Brazil in 1974-1975 and 1995-1996 showed that malnutrition decreased from 14.8% to 8.6%, stunting decreased from 19.5% to 2.4% while obesity increased from 4.1% to 13.9% in children aged 0-59 months (7,8). Another public health concern is deficiency in micronutrients, particularly iron deficiency anemia which affects major than 40% of children under 5 years (9-14).
Both under- and over-nutrition have adverse consequences in young children. Obesity is associated with a variety of health problems including diabetes mellitus type 2, hypertension, hyperlipidemia, asthma, sleep apnea, early malnutrition, lower self-esteem and psychological problems. Stunting is related to cognitive deficits and other development problems (2,15). Children with anemia in infancy are at risk for long-lasting developmental disadvantages such as retarded psychomotor development and impaired cognitive function (11,16-20).
The number of children in collective out-of-home day care has increased significantly all over the world (6,21). Since 1970, the number of day care centers in Brazil has increased considerably. In the state of São Paulo the level of teaching at daycare centers was the most growing one over the last years.
Recently, we have conducted a project “Efficient Daycare Center Project - Impact of Training Educators from Public/Philanthropic Daycare Centers on Hygienic-Dietetic Practices and on Health/Nutrition of Infants”(22). One of the objectives of this project is to identify the risk factors for nutritional problems and propose effective actions to improve nutritional status for children in these institutions. The current study is a part of this project with two objectives: 1) to document the prevalence of stunting, overweight and anemia in preschool children and examine if those nutritional problems are related and 2) to identify risk factors for these nutritional problems.
This is a cross-sectional study that uses baseline information from a survey conducted in eight daycare centers on the southern area of Sao Paulo city, Brazil in 2007.
The daycare centers were classified according to criteria of priority, which considered the existence of features of interest to the development of projects. The criteria in descending order of value were prioritizes: greater number of children in nurseries, number of educators, safety in the execution of research and rules of admission that the daycare centers only admit low income households. Consequently, the eight daycare centers that best met criteria were selected for the development of research.
All the children attending the nurseries of these eight daycare centers were included in the study. We excluded children with down syndrome (n=2), cerebral palsy (n=2), genetic syndromes (n=1), whose parents or guardians refused to sign the consent term (n=2) and children that weren’t on the day of the anthropometric data collection (n=3), totaling a loss of 3.6%. At the end, the study population was composed of 270 children.
Information on demographic, clinical, epidemiological, socio-economic and environmental variables was collected through interviews with the children’s mothers or guardians using a structured and pre-coded questionnaire. Children anthropometry including height and weight was measured using a pediatric digital scale and pediatric anthropometric rule. Children were weighed with pediatric digital model BP Baby Filizola, with minimum capacity of 125 grams, up to 15 kg and graduated every five grams. Children over 15 kg were weighed on portable electronic scale, Plenna®, capacity 150 kg, with a graduation of 100 in 100g. To measure the height was used anthropometric ruler of a movable cursor recommended by the Brazilian Society of Pediatrics graduated every 0.5 cm and the range of 0 to 120 cm. Anthropometric data of these children at birth were also obtained with the children’s card of birth.
Hemoglobin (Hb) concentrations were performed using portable hemoglobin HemoCue - ß Hemoglobin Photometer®, which is based on photometric reading with the use of ß hemoglobin disposable microcuvette. Anemia was defined as Hb concentrations less than 110 g/L (23).
All procedures for the interview, the anthropometry measurement and techniques to determine Hb levels were standardized and tested in the pretrial stage of the project.
Percentage of the life of the child in the daycare center (% of daycare attendance) was calculated by number of days the child spent in the daycare center divided by his/her age (in days) multiplied by 100. Data on height and weight were converted to z-scores of height-for-age (HAZ), weight-for-age (WAZ) and weight-for-height (WHZ) using WHO anthro software (24). The WHO standard reference was adopted to classify children nutritional status such as stunting (HAZ < -2), risk of stunting (HAZ < -1), wasting (WHZ < -2), risk of wasting (WHZ < -1), underweight (WAZ < -2), risk of underweight (WAZ < -1), and overweight (WHZ >1) (25). For measure of socioeconomic status (SES) was generated a classification using several variables such as mother’s occupation, quality of the house, household assets and facilities, water and sanitation. A socioeconomic index was created using principal components analysis according to the method used in Demographic Health Surveys and INCAP studies (26,27). Percapita income (monthly income divided by number of members in the family that live with this monthly income) was calculated in Real (local currency).
Descriptive procedures were applied to characterize the study population. Contingency tables and a log-linear model were used to investigate the co-occurrence of stunting, overweight and anemia. Univariate analysis was performed with different procedures such as t-test and chi-square. Multiple regression analyses were conducted to estimate the association of HAZ, WAZ, WHZ and Hb levels with their risk factors. Statistical analyses were conducted using SAS 9.2 (28). All statistical tests were two-sided tailed and significance was reported for p-values <0.05.
The present study was approved by Unifesp (Federal University of Sao Paulo) Ethics Committee in Research.
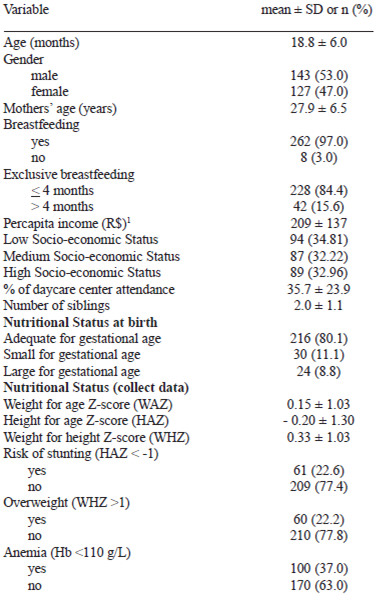
The general characteristics for the studied children are shown in Table 1. Of the 270 children who were 4 – 29 months of age (mean ± SD: 18 ± 6.04), 53% are boys and 47% are girls. Malnutrition prevalence was low (5,8% stunting, 2.22% underweight and 0.74% wasting), but the risk of malnutrition was high (22.6% for stunting, 14% for underweight and 8.9% for wasting). The prevalence of overweight was 22.2%. In our sample 37% of the children were anemic.
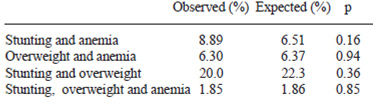
When data were treated as continuous variables, there were positive correlations between Hb levels and HAZ and WAZ, even controlled for age (Figure 1). For each 1g/L increased in Hb, HAZ scores increased by 0.013 and WAZ scores increased by 0.02. However, when data were treated as dichotomous variables, there was no significant difference between the observed and expected prevalence of children with two-way and three-way co-occurrence of risk of stunting, overweight and anemia (p>0.05 for all comparisons) (Table 2).

In univariate linear regression analyses (Table 3), there were significant association between Hb with age, number of siblings under 5 years old, percent of daycare attendance, and percapita income. Current anthropometric status only had positive association with the nutritional status at birth, but not with other variables. There was no association between current nutritional status or anemia with breastfeeding duration, exclusive breastfeeding, mothers’ schooling and gender (data not shown).
In a multiple linear regression analyses controlled for other confounders, similar associations were observed for Hb (Table 4). Hb levels increased by 0.61 g/L for each month increased in age; by 0.67 g/L for each 10% increased in daycare attendance; and by 2.4 g/L for each 100 reais. In contrast, Hb levels decreased by 3.15 g/L for each additional number of siblings. Again, current anthropometric status only had positive association with birth weight, but not with other variables. For each kg higher in birth weight, HAZ increased by 0.32, WAZ increased by 0.63 and WHZ increased by 0.62.
Currently, in urban areas in Brazil more and more people have access to healthcare. This means that diseases that had higher prevalence increasingly becomes less frequent. Furthermore, diseases that had low prevalence increasingly become more frequent.
Similar to many other developing countries in the world that have undergone a rapid demographic, epidemiological and nutritional transition, this study provides evidence that Brazil is going through a nutritional transition. The data shows low prevalence of malnutrition (wasting: 0.74% and underweight: 2.22%) and at the same time a high prevalence of children with overweight (22.23%) and risk of stunting (22.6%). The mean of HAZ in these children is negative showing a tendency to stature deficits.
Since anemia and malnutrition often share common causes, it is expected that multiple nutrition problems would co-occur in the same individuals. Our data showed that children with low Hb had also low HAZ and WAZ. However, the comparison of observed and expected values were not significant difference; it may due to loss of power when we categorized Hb, HAZ and WAZ as dichotomous variables.
Our results were not consistent with findings from some studies that showed the association between nutritional problems. For example, overweight has been shown associated with anemia (4, 29-31). In addition, stunting and overweight have been reported to coexist not only at the community level but also in the same household (32). These studies hypothesized that early malnutrition and nutritional deficiencies leading to stunted linear growth is related to important metabolic changes and increased risk of obesity later (2,29,33-35).
The present study showed high anemia prevalence (37% of our sample). These data are consistent with recent epidemiologic studies showing a very high prevalence of anemia among preschool children in big cities in Brazil and worldwide (9-11,16,18,36-39). Similar to other studies showing that anemia is more prevalent in children younger than 24 months, this study shows that age is an important risk factor for anemia (9, 40, 41). The lower Hb in younger children may due to the combination of the high demands for iron imposed by growth and the typical low intake of this nutrient, in quantity and bioavailability, (3,4,12,16,31,38,39). Many children are fed with available low-cost, energy-dense processed food (high in fat and sugars) and nutrient-poor foods which make them vulnerable to iron and other micronutrients deficiency (2,5,33,35,42).
In developing countries, the daycare centers are considered one of the strategies to improve growth and development of children from families with low socio-economic status. Children attending daycare centers have more opportunities to access to food in sufficient quantity and quality. Moreover, children can participate in various activities which promote adequate growth and development.
Our data showed a positive association between % of daycare attendance and Hb level. For each 10% increased in daycare attendance, Hb level increased by 0.67 g/L. Consistent with our study, Brotanek et al. (19) concluded that daycare/preschool attendance is protective against iron deficiency to US children. Konstantyner at al. (41) also showed a positive association between hemoglobin levels and the time the child attends in the daycare center in Sao Paulo city in Brazil. The minimum time of attendance in the institution has to be four months before the benefits are noticed. Therefore, daycare centers in low-income areas of cities as Sao Paulo and others poor cities may be important for reducing child anemia (9, 19). However, we didn’t find the association of the time the child attends in daycare center with other nutritional problems (underweight, stunting) as other authors observed (6, 43-46).
Simplified, effective and reproductive technologies are necessary to improve the health and promoting healthy living habits for children in developing countries.
There is specifically lack of financing policies to expand qualitatively and quantitatively the offer for daycare centers and preschools in Brazil. In view of the daycare centers as a protective factor for anemia and nutritional status, public policy should set priority to expand numbers of daycare centers and provide more resources to improve their services, particularly improving the quality of the diet offered by daycare centers. Findings from our and other studies suggested that the adoption of public policies for nutritional assistance can improve nutritional problems in preschool children.
Our findings showed positive association between birth weight with current nutritional status. Several studies from developing countries also report that birth weight not only influences postnatal growth during childhood but also have long term effect in the height of adulthood (47-49). Birth weight of children which reflect fetal growth in uterine is mainly determined by maternal nutrition status (50). Therefore, improving prenatal care and maternal nutrition status is an important strategy to prevent malnutrition. Children born as low birth weight are vulnerable for a greater number of infections which consequently cause a deficit of nutritional status, this fact leads that birth weight is directly related to the nutritional status early in life (51, 52).
In conclusion, this study provides evidence that the population, mostly children, in Sao Paulo city in Brazil are going through a nutritional transition with high prevalence of overweight, risk of stunting and anemia. Anemia is highly correlated with low height and weight for age. Attending daycare center appears to be an effective strategy to improve nutritional status for children from low income families. Therefore, the adoption of public policies to expand and improve services in daycare centers may help to prevent multi-nutritional problems in preschool children.
We would like to thank the members of the “CrechEficiente Project”, especially at his coordinator Prof. Dr. Jose Augusto de Aguiar Carrazedo Taddei, and the CAPES (Coordination of Improvement of Higher Education) by the exchange of practical training of doctorate abroad to the first author.
Recibido:13-05-2009
Aceptado: 09-03-2010