Introduction
Obesity is a condition of excessive accumulation of fat which compromises the health of the individual and is considered to be a feature of Food and Nutrition Insecurity across the world. The consequences of obesity on health are innumerable and varied, even to the extent of causing disability and thus having an adverse effect on quality of life (1).
A number of studies have reported that identification of the way fat is distributed across the body and of the type of excessive fat is more important than the quantification of total body fat (2).
Evidence has been found of an important association between abdominal adiposity and the development of morbidity (2-5). Abdominal fat is composed of subcutaneous and visceral fat. The latter is the principal fat to have been associated with metabolic disturbances and with the consequent development of morbidities, particularly with cardiovascular diseases (6-8).
The most appropriate methods for the identification of visceral fat are medical imaging techniques, such as computerized tomography (CT), which is considered the “gold standard” method, being the most precise, with the greatest accuracy and reproducibility. On the other hand, high cost and radiation exposure limit its use in clinical practice and in epidemiological studies (10, 11).
The study of alternative methods which are practical, low cost, non-invasive and offer accuracy and precision in the estimation of visceral fat are thus crucial.
Anthropometry is one of the methods whose validity in estimating this type of fat has been tested (2). However, few studies compare relationships between age groups, particularly in older adults, or primarily utilize a robust classification that guarantees representative equivalence in terms of quantity of visceral fat. The present study aimed to contribute to the identification of accurate and low cost methods which enable risk assessment and the prevention of cardiovascular diseases by assessing the sensitivity and specificity of waist circumference (WC), sagittal abdominal diameter (SAD) and waist-hip ratio (WHR) in predicting visceral fat in adults and older adults. This study thus extends and enriches the range of activities related to the food and nutrition security of populations.
Materials and methods
Patient recruitment
The study was carried out at the School of Nutrition of the Federal University of Bahia (UFBA) during the first trimester of 2009. One hundred and ninety-seven individual volunteers classified by sex, age and body mass (as per Figure 1) were recruited from the University Health Complex of the Federal University of Bahia and from the general community in the city of Salvador, Bahia, Brazil.
FIGURE 1
Sample Composition
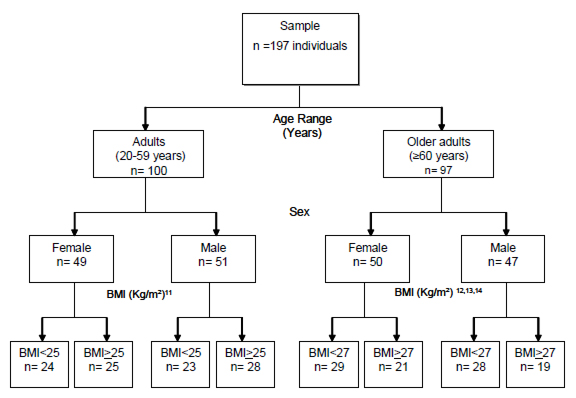
BMI: Body Mass Index
Exclusion criteria
Individuals <20 years old, with a BMI > 40 kg/m2; those who manifested severe malnutrition and disturbances (neural sequele, dystrophy), amputees or those with any form of problem that could compromise the verification of anthropometric measurements and the estimated accuracy of abdominal fat by CT were excluded from the study. Individuals who had recently undergone abdominal surgery, pregnant women or postpartum; individuals who had abdominal lesions and tumours, hepatomegaly and/or splenomegaly and ascites were also excluded.
Ethical aspects
All participants signed the Free and Informed Consent Form. The study did not involve procedures of high risk for the individuals involved and all received the test results, were seen at nutrition clinics and referred for health follow-ups, where necessary. The study was approved by the Committee for Ethics in Research of the School of Nutrition of UFBA (Judgement no. 01/09).
Data collection
A trained team collected the demographic and anthropometric data and a radiologist carried out the tomography test on all the individuals. For each individual the assessments (anthropometric and tomography) were undertaken on the same day, thus preventing oscillations in weight from interfering in the results.
Anthropometric assessment
Each individual’s measurements were taken by a trained anthropometric technician. Measuring techniques were standardized. Portable, digital scales (brand name Filizola, with a capacity of 150Kg at intervals of 100g) were used to measure weight with the individuals wearing light clothes and no shoes. Height was measured with a portable stadiometer (brand name SECA, TBW Importing Ltda.). Circumferences were measured with a metric tape made of inelastic synthetic material (TBW Importing Ltda.). Waist circumference was taken to be the minimum circumference between the costal margin and the iliac crest. Hip circumference was measured at the maximum protuberance of the buttocks, with the individuals wearing light clothes. The reading was taken to the nearest millimetre. BMI was calculated in kg/m2 and WHR by dividing each subject’s waist circumference by their hip circumference.
Sagittal Abdominal Diameter was verified with the help of a portable abdominal calibrator (Sliding-beam – Holtain, Ltd., Dyfed, Wales, U.K.) and measured with the individual lying down, with arms relaxed along the body and legs extended. The fixed caliper of the calibrator was placed under the individual’s back and the sliding caliper was brought up to the abdominal point between the iliac crests, at the level of the umbilicus. The reading was carried out to the nearest millimetre, at the end of expiration, according to the technique proposed by Kahn (15). The interclass coefficient was greater than 0.97.
Computerized tomography to assess the visceral tissue area
The computerized tomography was obtained using the Siemens Spirit Tomography of the Radiology Service at the University Hospital and analysed by an examiner. The test was carried out after 04 hours of complete fasting with the patient lying dorsal recumbent and with arms extended above the head. A lateral topogram was taken for precise identification of the location of the L4-L5, followed by a single axial tomography slice in this location, with slice thickness at 10 mm and time of exposure 3 seconds. Once the slice was obtained the external limits of the abdomen were characterised using a light pen cursor which measured the outer edges of the abdominal circumference and then calculated the total abdominal area (16).
After measuring the total abdominal area, the area of the visceral abdominal corresponding to the area of visceral fat was also outlined with a light pen cursor. This was determined by the demarcation of the abdominal cavity, taking as its limits the internal borders of the rectus abdominal, internal oblique and quadratus lumborum muscles, excluding the vertebral body and including the retroperitoneal, mesenteric and omental fat. The areas of fat were described in centimetres squared. The subcutaneous abdominal areas were calculated by subtracting the visceral abdominal fat from the total abdominal area (16).
Barite or organo-iodized contrasts were not used in the CT administration. A topography programme with radiographic parameters of 140 kV and 45mA was utilized for the abdomen examination. A density of -50 to -150 Hounsfield Units was used to identify the adipose tissue. An area of visceral tissue > 130 cm² was taken to signify an excess of visceral adipose tissue and to present risk for the development of cardiovascular diseases (17).
Statitical analysis
The Statistical Package for Social Sciences (SPSS) Version 11.5 was used for data processing. A descriptive analysis and a correlation test were undertaken, adopting a significance level of 5%. The coefficient of variation was calculated to assess the inter and intra examiner variability of the anthropometric measures. The distribution of continuous variables was verified by the Kolmogorov-Smirnov non parametric test. Pearson correlation was performed to assess the correlation of a normal distribution, and Spearman correlation for a non-normal distribution between the variables.
A Receiver Operating Characteristic Curve (ROC Curve) was constructed using a cut-off point for the reference test, that is, the area of visceral adipose tissue (VAT) measured by the CT. A 130 cm2 value (positive reference test) was selected as the threshold for excess VAT. In order to assess the performance of the anthropometric indicators, the sensitivity (probability of correctly detecting true positives) and the specificity (probability of correctly detecting true negatives) of each cut-off point were estimated and the cut-off point which produced the best combination of sensitivity and specificity was selected as the most appropriate value for indicator(s) of best prediction of a level of visceral adipose tissue area of 130 cm2, for each sex and each age group.
Results
Of the 197 individuals between 21 and 95 years old, there were a hundred adults with the mean age of men being 39.37 years (±13.08) and of women 39.93 years (±11.35). Of the ninety-seven older adults, the mean age of men was 72.19 years (±8.39) and of women 73.7 years old (±8.11).
As is seen in Table 1, the mean of waist circumference was higher in the older adults when compared to adults of the same sex. In relation to the SAD, we noted that the mean was higher in the group of older men (21.29 cm) while the lowest mean was seen amongst adult women (19.44 cm). The mean WHR was higher for men in both age groups.
TABLE 1
Descriptive analysis characteristics of the anthropometric indicators in adults and the older adults, Salvador, 2009
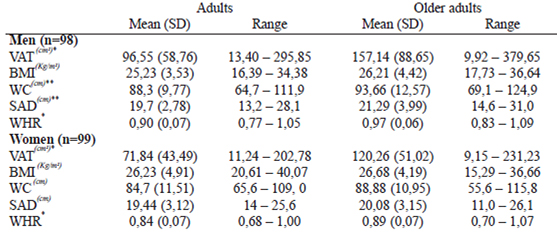
*p=0,000 ** p<0,05 SD: Standard Deviation; VAT: Visceral Adipose Tissue Area; BMI: Body Mass Index; WC: Waist Circumference; SAD: Sagittal Abdominal Diameter; WHR: Waist-Hip Ratio.
In relation to the visceral adipose tissue (VAT) area identified by CT, the mean was much higher in the older adults (157.14 cm2 for men and 120.26 cm2 for women). The lowest VAT area mean was found in adult women (71.81 cm2).
Although the mean BMI for adult men was similar to that seen in the older adults, a statistically significant difference between these two groups was found in the mean values for distribution of corporal fat and for VAT area. In the group of women, however, only the WHR and the VAT area presented statistical significance.
Table 2 shows the correlation between the anthropometric indicators and the CT-identified VAT area in both sexes in the adult and older adults. A highly significant correlation coefficient (p<0.001) was found between the SAD and WC anthropometric indicators and the abdominal visceral adipose tissue area in adult men and older men, and in adult women. For older women the correlation coefficient of these variables was slightly less, although highly significant. The SAD showed a highest correlation with the VAT area between the adults and older adults, similar to the correlation found between the WC and the VAT area. We noted that the WHR presented correlations of less than 0.70, except in the group of older men.
TABLE 2
Correlation coefficient between the anthropometric indicators and the CT-identified VAT area in the adult and older adults
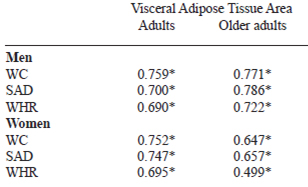
*p=0,000
WC: Waist Circumference; SAD: Sagittal Abdominal Diameter; WHR: Waist-Hip Ratio
Table 3 presents the cut-off points, sensitivity and specificity of the SAD, WC and WHR that identified a visceral adipose tissue area of >130 cm2 and the areas below the ROC curve for adults and the older adults of both sexes. We observed that the SAD cut-off points with the optimal combination of greatest sensitivity and greatest specificity were equal amongst male individuals (Adults – 20.2 cm; Older adults – 20.2 cm) and different amongst women (Adults – 21.0 cm; Older adults – 19.9 cm). The sensitivity and specificity for these cut-off points reach values that are considered high and are greatest for adults. The areas below the ROC curve were higher than 0.80 with values of p = 0.0000 (Figure 2).
TABLE 3
Cut-off points, sensitivity and specificity of SAD, WC and WHR that correspond to a VAT area of >130 cm2 and areas below the ROC curve for adults and older adults
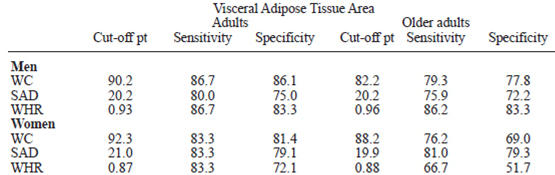
WC: Waist Circumference; SAD: Sagittal Abdominal Diameter; WHR: Waist-Hip Ratio; VAT: Visceral Adipose Tissue Area
FIGURE 2
ROC Curve to identify cut-off points for SAD, WC and WHR with a VATA of > 130cm², by sex and age – Salvador, 2009
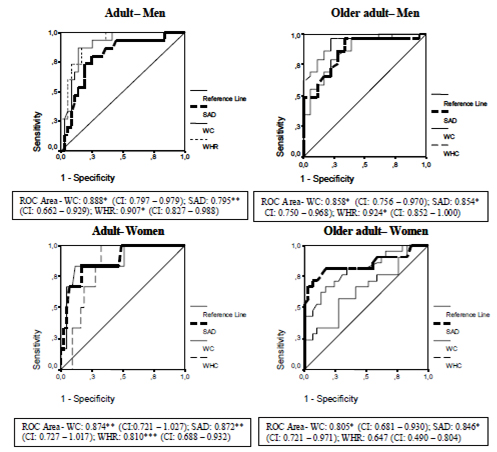
*p=0,000 **p<0,01 ***p<0,05 Sensitivity/Specificity/Reference line/WHR/SAD/WC
WC: Waist Circumference; SAD: Sagittal Abdominal Diameter; WHR: Waist-Hip Ratio; CI: Confidence interval (95%).
Regarding WC, we observed that the cut-off point of 90.2 cm and 92.2 cm for men (adults and older adults, respectively), identified a VAT area of >130 cm2, while the values found for the women were 92.3 cm and 88.2 cm. The sensitivity and specificity were higher in adults when compared to the older adults of both sexes. The WHR presented less sensitivity and specificity in identifying a visceral adipose tissue area of > 130cm2 in older women in relation to the other indicators.
Discussion
Over the years anthropometry has been shown to be an important indicator of total body mass and of body composition and has been tested as a method of estimating visceral fat because of the strict relationship between this type of fat and the development of cardiovascular events and other health risks. However, there are only a few research studies that assess the performance of anthropometric indicators in the identification of visceral fat area when compared to computerized tomography (2). This study not only carried out such a comparison but also investigated the differences between adults and older adults.
A classification by sex, age and body mass [using values of the cut-off points of BMI appropriate for each age group (11-14)] was undertaken to determine the inclusion of participants in the study. This guaranteed equivalence in the number of individuals in each group, enabling a better comparison of the results between these variables.
Our study demonstrated the high reliability of the anthropometric measures collected, with an interclass correlation coefficient greater than 0.97, which corroborates other studies (2,18). The collection of reliable data in studies which involve the use of anthropometry demand rigour in the standardisation of measuring techniques and in the training of the team.
All the means for the anthropometric measurements and for the visceral adipose tissue area observed in this study were greater in older adults. This may be explained by the BMI cutoff points adopted for the classification of body mass in older adults being higher than those for the adults. Moreover, the older adults are expected to have more abdominal fat, principally of the visceral type (19).
Most studies consider an area of >130 cm² of visceral adipose tissue as excessive, since it is associated with the development of cardiovascular diseases and other morbidities (17,20). A VAT area higher than this value was only found in older men. Sampaio et al (2), when studying a population between 20 and 83 years old, established an mean VAT area of 102.5 cm2 for men and 84.1 cm2 for women. Kim et al (21) studied individuals aged from 18 to 70 years old and found a VAT area mean of 159.8 cm2 in men and 127.4 cm2 in women.
Sagittal abdominal diameter is a new anthropometric measure and is practical, non-invasive, easy to execute, low cost and regarded as an important anthropometric indicator in estimating visceral adipose tissue (VAT) (2,4,10,22-25). In Brazil, there are few studies about SAD. We do not know the population values of this measurement and there is it still no consensus regarding the SAD cut-off point that evidences risk for the development of diseases. Some studies have found varied SAD mean in assessed groups. Sampaio et al (2) observed greater SAD mean in men (20.9 cm), as did Ohrvall (5) who, when assessing 845 individuals of both sexes aged between 19 and 66 years old, also noted a higher SAD mean in men (23.5 cm). This value was similar to that found by Turcato et al (35) in an assessment carried out on the older adults (23.0 cm).
Iribarren et al (23) measured SAD with the individual standing up and also found higher mean values in women (20.6 cm). The present study recorded mean SAD values according to sex and age which made it impossible to compare our findings with those of studies that carried out a more generalised analysis.
When analysing the correlation of the SAD with the visceral adipose tissue area, we noted that, as in other studies (2,4,5,22-25,27), the SAD measurement presented a high correlation with visceral adipose tissue measured by CT, which indicates that it is a strong predictor for this type of fat. We emphasise that this correlation was highest amongst older men.
In regards to the SAD cut-off points that identified a VAT area considered to present risk, this study encountered values close to those found in the literature. These SAD values have varied between 19 and 24 cm (2,3,15).
Waist circumference is a measurement that assesses cardiovascular risk and is also one of the criteria for defining metabolic syndrome. Its importance in the identification of obesity, as well as in the estimation of visceral fat, has been highlighted in the literature (21,28,29).
When analysing an individual’s WC in this study, we noted that this measurement’s mean values for adult women and older women already indicated risk for the development of metabolic complications associated with obesity, unlike the values found for men, who had WC values lower than the cut-off points defined as risk factors by the WHO (11). This last result was similar to that of a study carried out on older Brazilians which also found that WC values for both sexes were lower than the cut-off points that had been, until that point, considered to determine risk for this group (30).
For a given WC, abdominal adipose tissue distribution differs between the sexes. Furthermore, Kuk et al (28) showed that VAT accumulation for a given WC is also influenced by age and menopausal status.
WC measurement correlated very well with the VAT area in all the age and sex groups; the correlation was strongest in the group of older men. The study of Janssen et al (29), utilizing magnetic resonancing, found r=0.76 for women.
Similar findings were found in a study undertaken by Després et al (31) which recorded a correlation of r=0.82 between WC and CT-assessed VAT area in a study carried out on adult men. Kanda et al (32) noted a significant correlation both for men (r=0.78, p< 0.001) and for women (r=0.82. p< 0.0001).
In relation to the WC cut-off points that identified a VAT area defined as risk, we recorded values lower than those advised by the WHO (11) in men of both age groups (Adult=90.2 cm and Older adults= 82.2 cm). The values presented by the women in both groups, however, were above those of the WHO (Adult= 92.3 cm and Older adults= 88.2 cm). It is also important to stress that the cut-off points utilized to estimate a VAT area of > 130cm2 in the older adults of both sexes were lower. In other words, the present study proved that the cutoff points to assess WC as a predictor of the accumulation of visceral tissue in an older adults are lower than those of adults.
WHR, despite being considered one of the most common anthropometric indices for the assessment of body fat distribution, is not capable of differentiating between a deposit of visceral and subcutaneous fat (19). This may be explained by the increase in waist circumference and reduction in hip circumference that occurs with ageing.
When assessing the correlation between the WHR and the VAT area it was possible to observe that, compared to the other anthropometric measures previously cited (WC and SAD), the WHR presented the lowest correlation with this tissue, in each sex and age group. Others studies have found similar results, despite using different methodologies (33,34).
The WHR cut-off points of greatest sensitivity and specificity were higher in men from both age groups. Scheineider et al (35) assessed cardiovascular risk in individuals between 20 and 79 years old and encountered results similar to those found in our study, with WHR cut-off points of 0.95 and 0.85 for men and women respectively.
The classification by sex, age group and body mass, as well as the rigorous methodology applied, allowed us to robustly compare the findings for this population, guaranteeing equity between age groups in regards to classification characteristics and the greater reliability of the results. In summary, the anthropometric measures analysed here have good correlations with the visceral adipose tissue area for both sexes and age groups; of the three indicators, WHR had the lowest correlation; SAD showed the best correlation with the quantity of visceral fat amongst the older adults and WC demonstrated the best correlation for adults. Thus WC and SAD achieved the best performance in the identification of visceral fat considered at risk for the development of cardiometabolic diseases in adults and older adults.
These anthropometric indicators are therefore important tools in the professional health arena and may be included in health care protocols, both for individual assessment and population-based studies.
Acknowledgements
We gratefully acknowledge the contributions of Hospital Universit Teacher Edgar Santos, Salvador- Bahia, Brazil for their partner. This project was supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq).
Referencias
- Adams EJ, Grummer-Strawn L, Chavez G. Food Insecurity Is Associated with Increased Risk of Obesity in California Women. J Nutr. 2003; 133:1070–1074.
- Sampaio LR, Simôes EJ, Assis AMO, Ramos LR. Validity and Reliability of the Sagittal Abdominal Diameter as a Predictor of Visceral Abdominal Fat. Arq Bras Endocrinol Metab 2007; 51: 980 – 986.
- Risérus U, Ärnçov J, Brismar K, Zethelius B, Berglund L, Vessby B. Sagittal abdominal diameter is a strong anthropometric marker of insulin resistance and hiperproinsulinemia in obese men. Diabetes Care 2004; 27 (8): 2041-2046.
- Valsamakis G, Chetty R, Anwart A, Banerjee AK, Barnett A, Kumar S. Association of simple anthropometric measures of obesty with visceral at and the metabolic syndrome in male Caucasian and Indo-Asian subjects. Diabetes UK. Diabet Med. 2004; 21(12): 1339-1345.
- Öhrvall M, Berglund L, Vessby B. Sagittal abdominal diameter comparede with other antropometric measurements in relation to cardiovascular risk. Int. J Obes Relat Metab Disord. 2000; 24 (4): 497-501.
- Barroso SG, Abreu VG de, Francischetti EA. A participação do tecido adiposo visceral na gênese da hipertensão e doença cardiovascular aterogênica. Um conceito emergente. Arq Bras Cardiol. 2002; 27 (6): 618-630.
- Lemieux S, Després JP, Moorjani S, Nadeau A, Thériault G, Prud’homme D, et al. Are gender differences in cardiovascular disease risk factors explained by the level of visceral adipose tissue? Diabetologia 1994; 37 (8): 757–764.
- Seidel JC, Bakker CJG. Imaging techniques for measuring adipose-tissue distribution – a comparison between computed tomography and 1,5 magnectic resonance. Am J Clin Nutr. 1990; 51 (6): 953-957.
- Hirooka M, Kumagi T, Kurose K, Nakanishi S, Michitaka K, Matsuura B, et al. A technique for the measurement of visceral fat by ultrasonography: comparison of measurements by ultrasonography and computed tomography. Intern Med. 2005; 44 (8): 794-799.
- Van der kooy K, Seidell JC. Techniques for the measurement of visceral fat: a predicted guide. Int J Obes Relat Metab Disord. 1993; 17: 187–196.
- World Health Organization - Obesity Preventing and managing the Global Epidemic. Report of a WHO Consultation on Obesity. Geneva, WHO/NUT/NCD, 1998.
- American Academy of Family Physician. Nutrition Screening Initiative, NSI-2002. A Physician’s Guide to Nutrition in Chronic Disease Management for Older Adults. Leawood (KS): Am Acad. Family Physicians; 2002.
- American dietetic association. Position of the American Dietetic Association and the Canadian Dietetic Association: nutrition for physical fitness and athletic performance for adults. J Am Dietetic Association. 1993; 93 (6): 691-696.
- National Council of the Aging Inc. Committee on Diet and Health, Food and Nutrition Board, National Research Council. Diet and health implications for reducing chronic disease risk. Washington (DC): Nat Acad Press; 1989. 564-65.
- Kahn HS, Austin H, Williamson DF, Arensberg D. Simple anthropometric indices associated with ischemic heart disease. J Clin Epidemiol. 1996; 49:1017-24.
- Seidell JC, Oosterlee A, Thijssen MAO, Burema J. Assessment of intra-abdominal and subcutaneous abdominal fat: relation between anthropometry and computed tomography. Am J Clin Nutr. 1987; 45:7-13.
- Després JP, Lamarche B. Effects of diet and physical activity on adiposity and body fat distribution: implications for the prevention of cardiovascular disease. Nutr Res Rev. 1993; 6:137-59.
- Zamboni M, Turcato E, Armellini F, Kahn HS, Zivelonghi A, Santana H, et al. Sagittal abdominal diameter as a practical predictor of visceral fat. Int. J Obes Relat Metab Disord. 1998; 22(7): 655-660.
- Perissinotto E, Pisent C, Sergi G, Grigoletto F, Enzi G. Anthropometric measurements in the elderly: age and gender differences. Brit J Nutr. 2002; 87: 177–186.
- Lemieux S, Prud’homme D, Bouchard C, Tremblay A, Després JP. A single threshold of waist girth identifies normal weight and overweight subjects with excess visceral adipose tissue. Am J Clin Nutr. 1996; 64(5): 685-693.
- Kim JA, Choi CJ, Yun KS. Cut-off Values of Visceral Fat Area and Waist Circumference: Diagnostic Criteria for Abdominal Obesity in a Korean Population. J Korean Med Sci. 2006; 21(6): 1048-53.
- Petersson H, Daryani A, Risérus U. Sagittal abdominal diameter as a marker of inflammation and insulin resistance among immigrant women from the Middle East and native Swedish women: a cross-sectional study. Cardiovasc. Diabetol. 2007; 6:10.
- Iribarren C, Darbinian JA, Lo JC, Fireman BH, Go AS. Value of the Sagittal Abdominal Diameter in Coronary Heart Disease Risk Assessment: Cohort Study in a Large, Multiethnic Population. Am J Epidemiol. 2006; 164(12): 1150-1159.
- Smith DA, Ness EM, Herbert R, Schechter CB, Phillips RA, Diamond JA, et al. Abdominal diameter index: a more powerful anthropometric measure for prevalent coronary heart disease risk in adult males. Diabetes Obes. Metab. 2005; 7 (4): 370–380.
- Empana JP, Ducimetiere P, Charles MA, Jouven X. Sagittal abdominal diameter and risk of sudden death in asymptomatic middle- aged men: the Paris Prospective Study I. Circulation 2004; 110(18): 2781-2785.
- Turcato E, Bosello O, Francesco VD, Harris TB, Zoico E, Bissoli L, et al. Waist circumference and abdominal sagittal diameter as surrogates of body fat distribution in the elderly: Their relation with cardiovascular risk factors. Int. J Obes Relat Metab Disor. 2000; 24(8):1005-10.
- Duarte Pimental G; Portero-McLellan KC; Maestá N; Corrente JE; Burini RC. Accuracy of sagittal abdominal diameter as predictor of abdominal fat among Brazilian adults: a comparation with waist circumference. Nutr Hosp. 2010; 25(4): 656-661.
- Kuk JL, Lee S, Heymsfield SB, Ross R. Waist circumference and abdominal adipose tissue distribution: influence of age and sex. Am J Clin Nutr. 2005; 81:1330–4
- Janssen I, Heymsfield SB. Body mass index and waist circunference independently contribute to the prediction of nonabdominal, abdominal subcutaneous, and visceral fat. Am J Clin Nutr. 2002; 75: 683-688.
- Santos DM, Sichieri R. Índice de massa corporal e indicadores antropométricos de adiposidade em idosos. Rev Saúde Pública 2005; 39(2): 163-168.
- Després JP, Prud’homme D, Tremblay MC, Tremblay A, Bouchard C. Estimation of deep abdominal adipose tissue accumulation from simple anthropometric measurements to men. Am J Clin Nutr. 1991;54: 471-477.
- Kanda Y, Matsuda M, Hamamoto S, Fumiko K, Ko K, Michihiro M, et al. Analysis of waist circumference in Japanese subjects with type 2 diabetes mellitus: Lack of propriety to define the current criteria of metabolic syndrome. Diabetes Res Clin Pract. 2007; 77 (3): 220 – 223.
- Bouza A, Bellido D, Rodríguez, B, Pita S, Carreira J. Estimacíon de la grasa abdominal visceral y subcutánea en pacientes obesos a través de ecuaciones de regressíon antropométricas. Rev Esp Obes. 2008; 6 (3): 153-162.
- Garaulet M, Hernández-Morantel JJ, Tébar FJ, Zamora S. Anthropometric indexes for visceral fat estimation in overweight/obese women attending to age and menopausal status. J Physiol Biochem. 2006. 62 (4): 245-252.
- Schneider HJ, Glaesmer H, Klotsche J, Böhler S, Lehnert H, Zeiher AM, et al. Accuracy of Anthropometric Indicators of Obesity to Predict Cardiovascular Risk. J Clin Endocrinol Metab. 2007; 92(2): 589–594.