
The aim of this study was to describe the dietary patterns of pregnant women in northern Puerto Rico and explore associations between diet factors with pregnancy related measurements. This analysis is based on the Puerto Rico Testsite for Exploring Contamination Threats (PROTECT), a prospective cohort that is studying environmental risk factors for preterm births in PR. Participants completed a food frequency questionnaire (FFQ) around 20-28 weeks of gestation. The following pregnancy related measures were collected from the medical records: hemoglobin, blood glucose, blood pressure and gestational age. Potential associations between diet factors and pregnancy measures were assessed using chi square analysis with SPSS. A total of 180 participants completed the FFQ; low hemoglobin levels was found in 19.2%, high blood glucose levels was found in 21.1% by fasting blood glucose test and 24.6%by 1-hour 50 g oral glucose screening test, high blood pressure was found in 2.9% (systolic) and 6.5% (diastolic), and pre-term birth was found in 10.4% of the participants. High consumption of rice, desserts and sweets was associated with higher levels of fasting blood glucose levels (p<0.05), while high consumption of vegetables was associated with higher 1-hour glucose challenge test (p<0.05).No other significant associations were found. In conclusion, consumption of high dense energy food diets in pregnancy, such as rice, sweets and desserts, can lead to high levels of blood glucose and can be a potential predictor of other pregnancy complications during pregnancy in these study participants, such as gestational diabetes
Key words: Pregnancy, dietary patterns, pregnancy related measurements.
El objetivo de este estudio fue describir los hábitos alimentarios de mujeres embarazadas en Puerto Rico y explorar la asociación entre factores dietarios y medidas del embarazo. Este fue un análisis de datos basado en un estudio de cohorte prospectivo (PROTECT), que estudia los factores de riesgo ambientales para el embarazo pre-término en mujeres embarazadas. Las participantes completaron un cuestionario de frecuencia alimentaria (FFQ) en las semanas 20-28 de gestación. Los niveles de hemoglobina, glucosa en sangre, presión arterial y edad gestacional se recogieron de expediente médicos. Posibles asociaciones entre factores dietéticos y las medidas del embarazo fueron evaluadas usando Ji cuadrado en SPSS. Un total de 180 participantes completaron el FFQ; 19,2% tuvo bajos niveles de hemoglobina, 21.1% tuvo niveles altos de glucemia por prueba de glucosa en ayunas y 24,6% por prueba de tolerancia a la glucosa de 1 hora; la hipertensión arterial fue encontrada en 2,9% (sistólica) y 6,5% (diastólica) y nacimiento prematuro fue encontrado en 10,4%. Un alto consumo de arroz, postres y dulces se asoció con mayores niveles de glucosa en ayunas (p<0,05), mientras que el alto consumo de vegetales se asoció con mayor nivel de la prueba de tolerancia a la glucosa (p<0,05). No se encontró ninguna otra asociación significativa. En conclusión, el consumo de alimentos de alta densidad energética en el embarazo como arroz, postres y dulces pueden elevar los niveles de glucosa en sangre, lo cual puede ser un predictor potencial de complicaciones en el embarazo en estas participantes, como diabetes gestacional.
Palabras clave: Embarazo, hábitos alimentarios, medidas relacionadas al embarazo.
Graduate School of Public Health, Medical Sciences Campus, University of Puerto Rico.
Adequate nutrition is important in all life stages, but in pregnancy, is critical to the mother and the fetus. Good nutrition should start in the pre-conceptional period and continued throughout pregnancy in order to optimize health and reduce the risk of pregnancyrelated complications. Maternal nutrition during pregnancy has been shown to have a large positive as well negative influence in pregnancy, including gestational duration, onset of gestational diabetes, hypertension and other outcomes (1).
Globally, almost half of pregnant women have iron deficiency (2) and it has been estimated that gestational diabetes (GDM) affects more than15% of pregnant women(3), while preeclampsia affects 5-10% of pregnancies and is responsible for approximately 50,000 maternal deaths per year worldwide (4). Additionally, nearly15 million infants are born prematurely throughoutthe world, and the US is one of the top ten countries with higher numbers of pre-term births (5). In Puerto Rico, the prevalence of anemia in the third trimester of pregnancy is high, reported at41%in 2009 (6). Hypertension was found in 43.9% of women of 18 years and older in 2013(7). The prevalence rate of GDM in Hispanics in the US is among the second highest compared to other ethnic groups (8). Prematurity among Puerto Rican women living in the U.S. in 2010 reached 13.5% (5), while among women residing in Puerto Rico, during the same year, the prematurity rate was higher, reaching 16.7% (9).
Diet plays an important role and it is a modifiable factor for reducing the risk of some pregnancyrelated complications. Studies have found that high energy consumption, together with a high intake of carbohydrates (i.e. refined foods),are dietary risk factors for the development of GDM, while foods low in refined carbohydrates and high in fiber reduce hyperglycemia and also reduce the risk of cesarean deliveries (10). In addition, diets high in cereals, refined carbohydrates, sugar sweetened beverages, processed meats and salty snacks are directly associated with pre-eclampsia (11-13) while use of calcium supplements (14) and folic acid (15) is inversely associated with pre-eclampsia. With respect to preterm delivery, regular fish consumption and use of calcium supplements has been shown to reduce its risk (16), while coffee consumption, sugar-sweetened beverages and the use of artificial sweeteners increases its risk (17, 18). Furthermore, studies show that anemia is inversely related to red meat consumption and use of vitamin C and iron supplements (19).
Little is known about the role of dietary patterns in Hispanic pregnant women and no study has assessed the association between dietary patterns and pregnancy-related measurements in Puerto Rican women. Therefore, the aim of this study was to describe the dietary patterns in Puerto Rican pregnant women and analyze the association between specific protective and non-protective diet factors and pregnancy related measurements, such as blood glucose, blood pressure, hemoglobin levels and gestational age. Results from this study could help design interventions to improve the diet quality of Puerto Rican pregnant women.
PROTECT is a prospective cohort study that recruits pregnant women residing in the northern karst area of Puerto Rico to be followed to completion of pregnancy. Its primary aim is to examine the role of environmental factors, such as phthalates, on the risk of preterm pregnancies. Eligible study subjects are healthy pregnant women 18 to 45 years of age, who reside in a municipality of the northern karst area of Puerto Rico are less than 20 weeks gestation, plan to deliver in a participating hospital, and do not have any of the study exclusion criteria (described below). Most pregnant women are recruited on or before 12 weeks gestation. Data are collected through questionnaires administered at three intervals of gestation, 16 to 20 weeks, 20 to 24 weeks, and 24 to 28 weeks. Biological samples are also obtained at those three pregnancy intervals and research nurses conduct interviews using standardized questionnaires. Medical records are reviewed and data abstracted at the same intervals and following completion of pregnancy.
PROTECT aims to recruit 1,800 pregnant women, which would provide sufficient statistical power to detect an association between phthalate levels and the risk of preterm. No estimates of power were made for this secondary analysis because it is an exploratory study about possible associations between maternal diet factors and hemoglobin levels, glucose tolerance, blood pressure and gestational age among a group of Hispanic women. The study was approved by the MSC-UPR Institutional Review Board and all participants provided written consent to participate in the study.
At the moment this secondary analysis was performed, a total of 721 pregnant women had been recruited and followed by the PROTECT program from February 2011 to February 2014. Potentially eligible study subjects were screened for exclusions to participation that include a history of specific pregnancy complications, such as threatened abortion, vaginal bleeding or severe abdominal pain (undiagnosed), diabetes, heart disease, liver disease diagnosed before pregnancy, high blood pressure, nephropathy, neuropathy and surgery during the current pregnancy. Other exclusion criteria included: (a) taking oral contraceptives less than three months before conception; (b) current pregnancy resulting from assistive reproductive technology and; (c) having a chronic medical condition under treatment, or a pregnancy complication, such as placenta previa. These analyses included a total of 180 study subjects that had completed their pregnancy and had completed the Food Frequency Questionnaire (FFQ).
The PROTECT pregnancy follow up includes administering standard questionnaires at three specific gestational window, Visit 1 (16-20 weeks), Visit 2, (20-24 weeks), and Visit 3 (24-28 weeks). The questionnaires for visits 1 and 3 were administered during prenatal care visits at the clinic; visit 2 was conducted during a home visit. In addition, medical record data abstraction by trained personnel was conducted during all three gestational windows and for labor and delivery. The questions used in the PROTECT questionnaires were derived from previously field-tested surveys, the National Health Interview Survey, the National Health and Nutrition Examination Survey (NHANES), and the Birth Defects Prevention Study. All three had Spanish versions that have been field-tested as well.
First Visit: This questionnaire obtained data on socio-demographic characteristics of the mother, such as years of maternal education and family annual income. For this study it was categorized as <$20,000 or ≥$20,000, based on the poverty index by size of family and number of related children <18 years in 2012 in Puerto Rico.
Second Visit: A semi-quantitative FFQ was provided to the participants to be completed at home and to bring back during the third visit. Participants also completed other questionnaires for the main study.
Third Visit: The FFQ was collected and a third questionnaire on prenatal exposures and complications was administered. At this visit, key data abstracted from the medical record included hemoglobin and blood glucose levels.
Delivery and Postpartum: Data abstracted from the medical record included date of delivery and gestational age.
Anemia: Anemia was defined as hemoglobin level <11 g/dL, following the World Health Organization criteria, and based on maternal hemoglobin levels obtained at 16-20 weeks of pregnancy (2).
Glucose metabolism: Results from the glucose challenge test (GCT) and fasting glucose tolerance test (FBS) were taken from medical records, which are routinely measured at 24-28 weeks of gestation to identify women who may have gestational diabetes. GCT was categorized as adequate levels (<140 mg/dL) or high levels (>140 mg/dL) and FBS as adequate levels (<95mg/dL) or high levels (>95 mg/dL).
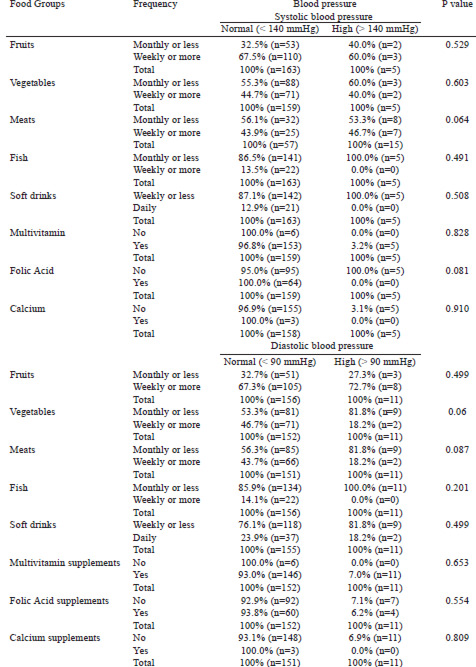
Blood pressure levels: these were taken from the medical record in the last routine prenatal visit. High systolic blood pressure was defined as >140 mmHg and high diastolic blood pressure as >90 mmHg.
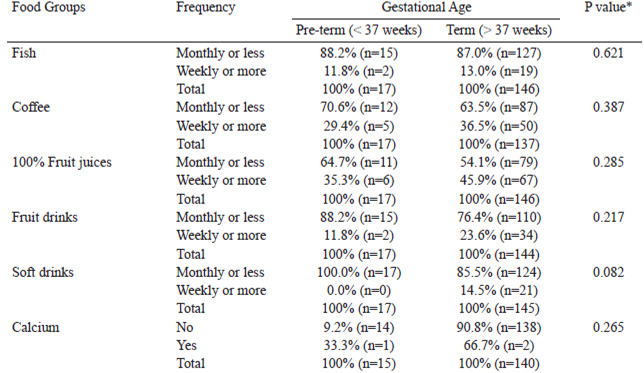
Gestational Age: Pre-term birth was defined as a gestational age less than 37 weeks (5). In the 80% of subjects with a sonogram prior to 20 weeks, the gestational age was based on the sonogram, for the remainder, gestational age was based on the reported last menstrual period. These data were obtained from the medical records abstraction.
A semi-quantitative FFQ to assess the dietary patterns was given to participants in the second visit to complete at home and bring back at the third visit. This FFQ was validated for its use in Puerto Ricans adults living in Puerto Rico (20). It was modified and adapted from the original FFQ developed for Puerto Ricans living in Boston, Massachusetts (21). The data obtained were the summary questions of the following food groups and supplements: fruits, vegetables, fish, cereals, dairy products, red meat, sugar-sweetened beverages, calcium, iron, vitamin C and multivitamin containing folic acid, which were examined in this analysis.
Univariate analysis was performed in terms of means and standard or percent deviation to describe the socio demographic factors (age, education and annual household income) and measures related to pregnancy (hemoglobin, fasting glucose, glucose 1 hour, blood pressure and gestational length).
To describe the dietary factors of the participants, the percentage frequency of consumption (daily, weekly or monthly) of the following food groups was used: fruits, vegetables, fish, meat, cereals, grains and starchy vegetables, rice, sweets, milk, coffee, juice 100% natural, fruit drinks, sweetened beverages and supplements use like calcium, iron, folic acid, multivitamins and vitamin C.
Continuous variables were categorized for use in bivariate statistical analysis. Bivariate analyses were performed to analyze the association between frequency of consumption of selected food groups and measures related to pregnancy. The chi-square of Pearson or Fisher's exact test was performed if any of the expected cell was less than 5 was used.The statistical program SPSS version 20 with a significance level of p <0.05 was used.
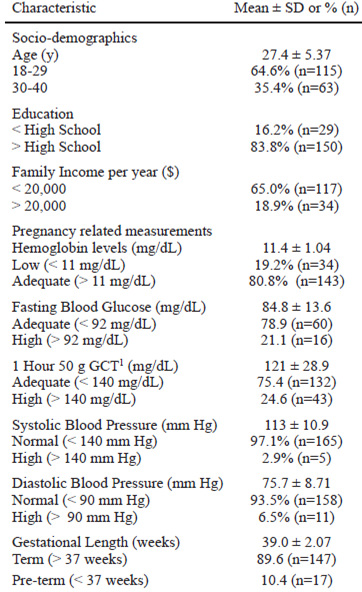
Most participants in this analysis were 18-29 years old (64.6%), had completed a high school degree (83.8%) and had an annual income below $20,000 per family (65.0%; Table 1). Low hemoglobin levels was present in 19.2%, high blood glucose levels was found in 21.1% using FBS and 24.6% using GCT, high blood pressure was found in 2.9% using systolic and 6.5% using diastolic as the reference method. Among all participants, 10.4% were born preterm (Table 1).
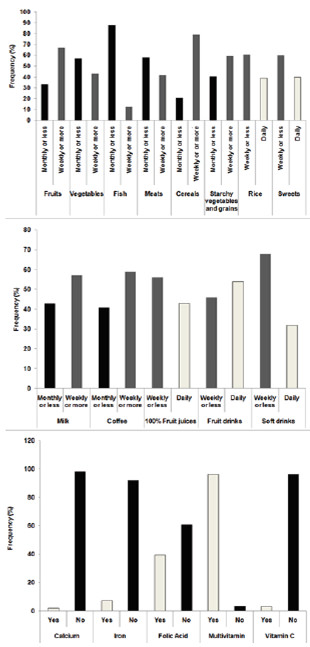
Most participants consumed fruits, starchy vegetables, grains, and milk weekly or more frequently, while most consumed vegetables, fish and meat monthly or rarely. Rice and desserts and sweets were consumed by most weekly or less frequently. Milk, coffee, 100% fruit juices and soft drinks were consumed by most weekly or more frequently, while fruit drinks were consumed by most with a daily frequency. Almost all of the participants used multivitamins, while the use of calcium, iron, folic acid and vitamin C individually was very low (Figure 1).
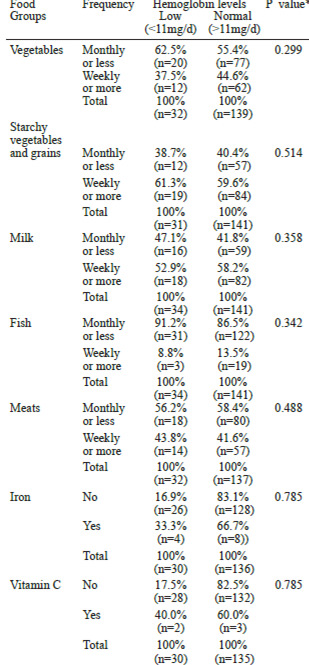
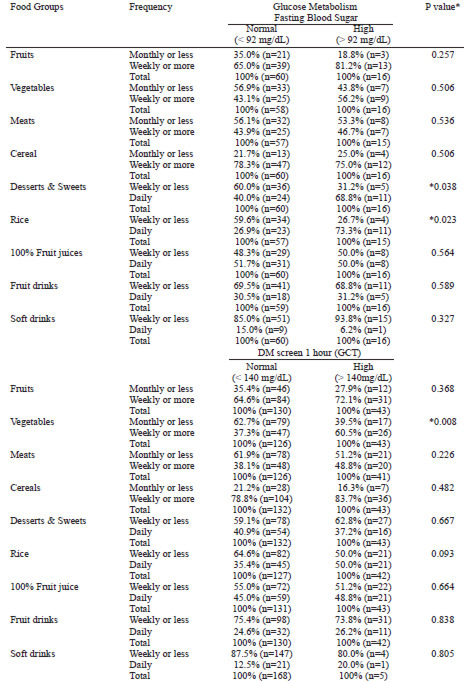
No significant associations were observed between any of the diet factors studied and hemoglobin levels (Table 2). No significant associations were observed between fruits, vegetables, meats, cereals, 100% fruit juices, fruit drinks and soft drinks with fasting glucose levels (Table 3). Women who consumed desserts and sweets daily were more likely to be classified as having high fasting glucose levels(68.8%), compared to those women who consumed these foods less frequently (31.2%; p=0.038). Similarly, women who consumed rice daily were more likely to be classified as having high fasting glucose levels (73.3%) compared to those women who consumed these foods less frequently (26.7%; p=0.023). In the case of 1-hour GCT, women who consumed vegetables weekly or more frequently were more likely to have higher glucose levels (60.5%), compared to those who consumed vegetables monthly or less frequently (39.5%, p=0.008) (Table 3)
No significant associations were observed between the consumption of the foods studied and high systolic or diastolic blood pressure. Also, no associations were found between blood pressure and the frequency of consumption of the following foods: cereal, milk, 100% fruit juice and fruit beverage (data not shown). However, a marginally significant association was observed with consumption of meats, whereas those who consumed meats monthly or less frequently were more likely to have higher systolic blood pressure (53.3%), compared to those who consumed meats more frequently (46.7%; p=0.064). In addition, those who consumed vegetables monthly or less frequently were more likely to have high diastolic blood pressure levels (81.8%), compared to those who consumed vegetables more frequently (18.2%, p=0.060) (Table 4). No significant associations were observed between the diet factors studied and gestational age (Table 5).
These analyses showed that daily consumption of desserts, sweets, and rice, were associated with higher fasting glucose levels, while consumption of vegetables weekly or more frequently was associated with higher 1-hour GCTlevels, but no significant associations were detected between the diet factors studied and hemoglobin, blood pressure or gestational age in this group of pregnant women.
Only a small percent of the sample had low hemoglobin levels, which was lower compared to a PNSS report in 2009 (6), in which 41% had anemia (low hemoglobin levels). On the contrary, we found a higher prevalence of high glucose levels in the present sample compared to data from NHANES in Mexican-American women aged 20-39 years, which was 12.0% (22). High blood pressure levels in the present sample was also much lower compared to the report from the BRFSS in 2013 (7), in which 43.9% of women of 18 years and older reported to have high blood pressure levels. Similarly, pre-term birth was lower compared to data reported in Puerto Rican women, which have reported levels as high as 16.7% (9).
In this study, women who consumed desserts, sweets and rice daily were more likely to be classified as having high fasting blood glucose levels. This can be explained by the high glycemic index (GI) values of these foods. The GI relates to how much a food raises blood sugar. Consumption of white rice as a staple food is a risk factor for developing diabetes and metabolic syndrome in adults from Puerto Rico (23). These results are consistent with studies in Asian pregnant women (24) and in Hispanic women (25), in which consumption of high-energy group foods, such as carbohydrates and energy-dense snacks was a risk factor for the development of GDM. In addition, a study in a group of Hispanic pregnant women with GDM that received an intervention diet to limit energy intake and increase consumption of complex carbohydrates and low GI foods for 4 months, found that consumption of low glycemic foods could help to control glucose levels in plasma as well as GDM (10). We also found that women who consumed vegetables weekly or more frequently were more likely to be classified as having high levels of 1-hour oral glucose challenge test. These results are not consistent with other studies (26). A possible explanation is that most of the vegetables consumed by participants were lettuce, tomato, onion and corn. Some of these vegetables have more sugar and less fiber, and therefore, a higher GI compared to other vegetables with lower GI and higher fiber content. For example, sweet corn has a mean GI of about 60. In addition, in individuals with type 1 diabetic, consumption of lettuce and tomatoes did not improve blood sugar levels compared to other high fiber vegetables, such as broccoli, artichokes and mushrooms (27). More research is needed to differentiate the type of vegetables consumed and cooking methods in these associations.
We did not find an association between consumption of vegetables, starchy vegetables and grains, milk, fish, meat and supplements use, such as iron and vitamin C, with hemoglobin levels. Other studies have found that the consumption of fish and lean red meats were inversely associated with the development of anemia (28), as well iron and vitamin C supplementation (19). In addition, we did not find an association between consumption of fruits, cereal, meats, fish, milk, sugar sweetened beverages and use of multivitamins and folic acid supplements with blood pressure levels. On the contrary, other studies have found that a higher consumption of cereals (4), sugar-sweetened beverages (13), and red meats (12) are directly associated with higher blood pressure levels, while consumption of fruits and vegetables (12), fish (29) and folic acid and multivitamin use (15) are inversely associated with higher blood pressure levels. A recent study in 191 Brazilian pregnant women, in which three major dietary patterns were found in the sample (healthy, processed or typical), no associations were found with any of the patterns and blood pressure during pregnancy but those consuming less processed foods had lower systolic blood pressure post-partum (30). However, in the present study, a marginal significant association (p=0.060) was observed in that those consuming vegetables less frequently were more likely to have higher diastolic blood pressure levels. These findings are consistent with other studies (12).
With respect to gestational age, we did not find significant associations with the consumption of fish, coffee, sugar-sweetened beverages and calcium supplementation and this variable. Other studies have found that consumption of fish (16) and calcium supplementation (14) are associated with longer gestational period and reduction in the risk of pre-term birth, while consumption of coffee (17) and artificial sweetened beverages (18) are associated with preterm delivery.
A possible explanation for the lack of associations between the frequency of consumption of these food groups and some of the pregnancy related complications measured in this study is that participants may have sub-reported food consumption in the questionnaire as it was self-administered. Also, the questionnaire did not allow distinguishing if the food was fresh or frozen, or which type of cooking method was used, which was a limitation of this study. In addition, many women did not complete the FFQ. Furthermore, most participants were healthy, so the number of participants experiencing any abnormal levels in the outcomes studied was rather low. Also, the use of a convenience sample and the crosssectional design of our study does not allow us to infer causality or to generalize our findings to other groups of pregnant women.
In conclusion, high consumption of rice and desserts and sweets, which are high glycemic foods, were associated with higher blood glucose levels. In this Hispanic population, white rice is a main staple of the diet. Therefore, interventions in Puerto Rico should target reducing white rice consumption, as well as desserts and sweets, during pregnancy for controlling blood glucose levels. With simply exchanging refined carbohydrates with their whole grain version, which are lower in their glycemic index and higher in their fiber content, many pregnant women could maintain blood sugar at optimal levels, which could potentially help reduce development of GDM. However, more studies are needed to confirm these results.
Funding source: Supported by award P42ES017198-01A1 (Superfund Research for the National Institute of Environmental Health Sciences) and in part by awards G12RR03051 (RCMI Clinical Research Center), 5G12-MD007600 (Center for Collaborative Research in Health Disparities), and U54MD007587 (Puerto Rico Clinical and Translational Research Consortium) from the Institute on Minority Health and Health Disparities, National Institutes of Health
Recibido: 14-11-2014
Aceptado: 28-02-2015