
The Objective this study is to compare the consumption of artificial sweeteners by sex and BMI status among university students in Peru, Chile, Guatemala and Panama. Survey of consumption of artificial sweeteners containing foods was designed and applied, adapted for each country with pictures of surveyed foods. After the survey application, a total of 1,229 participants male and female both university students from 4 different Latin American countries: Chile (n=473); Panama (n=300); Guatemala (n=253); Peru (n=204) were submitted to a anthropometry measeurement. Over 80% of students ate at least 1 food that contained artificial sweeteners, acesulphame-k, sucralose, and aspartame had the highest levels of consumption. Females in Chile and Guatemala ate the most sucralose (25.7 (6.6-50.9), p<0.05; 38.3 (15.1-82.5). Males in Panama ate the most acesulphame-k, (35.3 (11.5-91.5), p<0,05). Females had a positive correlation between artificial sweetener consumption and BMI for: acesulphame-k, aspartame and cyclamate. Males had a negative relationship between acesulphame-k, aspartame and BMI (p<0.05). We found a high consumption of artificial sweeteners among both male and female Latin Americ an university students, with differences by country, sex and BMI status.
Key words: Artificial sweeteners, estimated intake, nutritional status, acesulphame-k, saccharin.
El objetivo del estudio es comparar el consumo de edulcorantes artificiales no nutritivos por sexo y estado nutricional (IMC) entre los estudiantes universitarios en Perú, Chile, Guatemala y Panamá. Se diseñó y aplicó una encuesta de consumo de alimentos que contienen edulcorantes artificiales no nutritivos, adaptado para cada país con fotos de alimentos encuestas. Posteriormente se aplicó la encuesta y una evaluación antropometrica entre 1.229 estudiantes universitarios en 4 diferentes países de América Latina: Chile (n = 473); Panamá (n = 300); Guatemala (n = 253); Perú (n = 204). Más del 80% de los estudiantes comía al menos 1 alimento que contiene edulcorantes artificiales, acesulfamo-K, sucralosa, aspartame y tenían los niveles más altos de consumo. Las mujeres en Chile y Guatemala comsumieron más sucralosa (25,7 (6,6-50,9), p <0,05; 38,3 (15,1-82,5). Los hombres de Panama comsumían más acesulfamo-K, (35,3 (11,5-91,5), p <0,05) Las mujeres tenían una correlación positiva entre el consume de edulcorante artificial y el IMC para: acesulfamo-K, aspartamo y ciclamato hombres tenían una relación negativa entre el acesulfamo K, aspartamo y el IMC (p <0,05). Encontramos un alto consumo de edulcorantes artificiales entre los estudiantes de ambos sexos en las universidades de América Latina, con diferencias por país, sexo e IMC.
Palabras clave: Edulcorantes no nutritivos, ingesta estimada, estado nutricional, acesulfame-k, sacarina
Facultad de Ciencias de la Salud. Universidad San Sebastián. Chile. Facultad de Salud. Universidad Santo Tomás, Viña del Mar, Chile. Universidad de San Carlos, Guatemala City, Guatemala. Universidad Interamericana de Panama. Panama. Universidad Nacional Mayor de San Marcos, Lima, Perú.
Artificial sweeteners are food additives that have the ability to simulate the presence of sugar in food (1). These sweeteners are available across the primary food markets of the world and are added to many different types of foods.
Additionally, because these sweeteners have little or no calories they have high consumer acceptance, as many consider them to be healthy and help maintain weight (2). Artificial sweeteners have been available since the late 1800s. More recently the consumption of these types of sweeteners has increased in many countries. Saccharin, cyclamate, aspartame, acesulphame-k (or acesulphame potassium), sucralose, neotame, alitame and stevia are among the most common artificial sweeteners.
The first three substances: saccharin, cyclamate, aspartame are known as first generation sweeteners. After which came second generation sweeteners , which include acesulphame-k, sucralose, neotame, alitame that have different market inflection points(3).
Cyclamate was discovered in the United States in 1937. This sweetener is sodium and calcium cyclamic acid and has high water solubility. It is 30-50 times sweeter than sugar. As it is a less intense sweetener, it is mixed with sodium saccharin in order to increase its sweetening effect (3).
Saccharin is the oldest artificial sweetener. Saccharin is a sulphonamide, whose hydrogen atom is somewhat acidic and readily forms salts. Sacchairne is approximately 300 times sweeter than sugar and has zero calories (1).
Aspartame was discovered in 1965. It is an artificial sweetener comprised of a methyl ester of a dipeptide formed by the L - aspartic acid and L - phenylalanine. It is 180 to 200 sweeter than sugar and has 4 calories per gram (4).
Acesulphame-k is 200 times sweeter than sugar. It was discovered in 1967 and chemically composed of the potassium salt of 6-methyl-1,2,3-oxathiazine-4 (3H)-one 2,2-dioxide. It is a stable sweetener that has good water solvability, although at high concentrations it has a bitter taste. It cannot be metabolized and is thus secreted, without any change, in the urine (4).
Sucralose is an artificial sweetener discovered in 1976 composed of 1.6 dichloro - 1,6 dideoxy - β-D-fructofuranosyl - 4 - chloro - 4 deoxy - αD - galactopyranoside obtained by selective halogenation of the sucrose molecule. It is 600 times sweeter than sugar and has no calories (4).
Stevia is a subtropical jungle plant from the highlands of Paraná is also native to the northeast region of Misiones, Paraguay where the indigenous people use it for medicinal purposes. The stevia plant produces a natural sweetener, 300 times stronger than sucrose with no calories. Its leaves can be used in a natural form and because of its strength as a sweetener only a small amount is needed (5, 6).
The use of artificial sweeteners has been associated with health lifestyles, including maintaining weight within the normal range. Advertisements for healthy foods that contain artificial sweeteners have increased and have the power to influence young consumers, who use these sweeteners for weight maintenance and because of family environment (7).
Despite the increase in use of artificial sweeteners in food, little or nothing is known about the consumption of artificial sweeteners among young people in Latin America. The aim of the study was to compare the consumption of artificial sweeteners among a sample of university students in Peru, Chile, Guatemala and Panama.
Cross-sectional studies. We studied 1,229, male and female university students (public and private universities) between the ages of 18-26; among which 472 were from Chile (private), 300 from Panama (private), 253 from Guatemala (public) and 204 from Peru (public), the implementation of the surveys was between June and November 2014. The sample size for each country was calculated based on a study by Arcella (8) with a 95% confidence interval and 90% power and precision calculated as observed sample size – recommended value. The study had a non-probabilistic.
The criteria of inclusion used in the study were; being a university student with metabolic diseases and type 1 diabetes and those who did not complete the data entry forms were excluded (were excluded students for not having completed all information). Students were asked to sign an informed consent and over 27 years old. The study protocol was reviewed and approved by the IRBs at the different university sites. The study was developed following the Helsinki Declaration with respect to studies conducted with human subjects and was approved by the local ethics committee beings. Finally the compliance with STROBE has been addressed in this study.
Foods that contain artificial sweeteners and liquid and powdered sugar substitutes were sampled in each country through visits to markets. Each product was photographed and numbered. The survey contained sweetener a)milk products (yogurt, milk, etc), b)breakfast cereals, granola bars, c) liquid and powdered juices, d) carbonated beverages and energy drinks, e)cookies, f) flan/custard, jello, and g) sugar substitutes used to sweeten coffee and tea (tablet and liquid forms). A total of 122 products were sampled in Chile, 109 in Panama, 29 in Guatemala, and 124 in Peru.
To determine the consumption of artificial sweeteners, a survey of weekly food consumption was adapted for each country (only foods that contain artificial sweeteners were asked).
The survey was analysed using Excel. For the analysis of the survey, we considered type and amount of each artificial sweetener determined by the additives listed on the nutritional label per 100 g or ml.
Weight was measured using an electronic precision scale (GAMMA ®) with sensitivity of 0.1 kg, which allowed consumption per kilo of weight to be calculated. Height was measured with a stadiometer attached to the scale. Nutritional status was determined using body mass index (BMI), calculated as weight (kg) / height2. Normal BMI was defined as 18.5-24.9; overweight 25.0-29.9; and obesity >= 30 kg/m2
.Data were analysed using an Excel spreadsheet and SPSS 19.0. To evaluate the normality of continuous variables (age, weight, height, and consumption of artificial sweeteners) we used the Shapiro Wilk goodness of fit test. For comparisons by sex we used Student t or Mann-Whitney for normally and non-normally distributed variables, respectively. To compare by country we used either ANOVA or Kruskal-Wallis tests. For correlations we used Pearson or Spearman correlations depending on the normality of the variable. For all tests p<0.05 was considered statistically significant
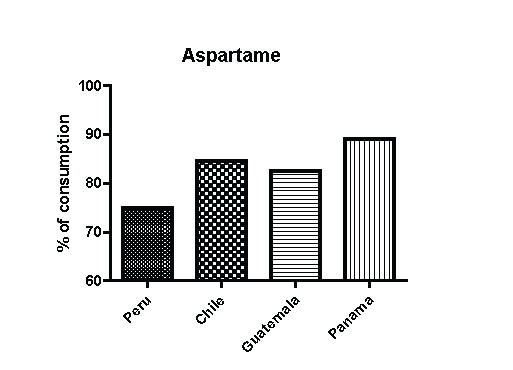
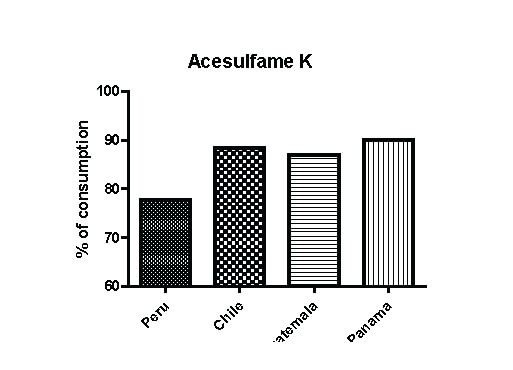
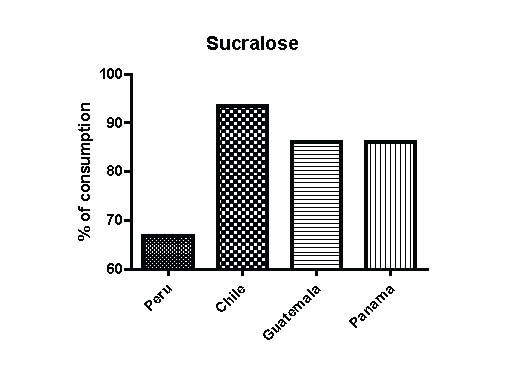
The sample consisted of 1,229 university male and female students of different majors: health, education, engineering, law. Over 80% of the sample consumed at least 1 food per day that contained an artificial sweetener. The sweeteners with the highest intake were acesulphame-k, sucralose, and aspartame (Figure 1,2 and 3), 9.3% of students in Peru consumed stevia, compared to 1.9% in both Panama and Chile. Cyclamate and saccharin were only consumed in Chile, among 23% and 25.8% of students, respectively
Comparing consumption (Table 2,3) between countries (kilos of weight), we found significant differences women in Guatemala have the highest consumption of acesulphame-k (p<0.05), Chile women show the highest consumption of sucralose (p<0.05), Panama women show the highest consumption of aspartame (p<0.05). For Panama men have the highest consumption of acesulphame-k and aspartame (p<0.05).
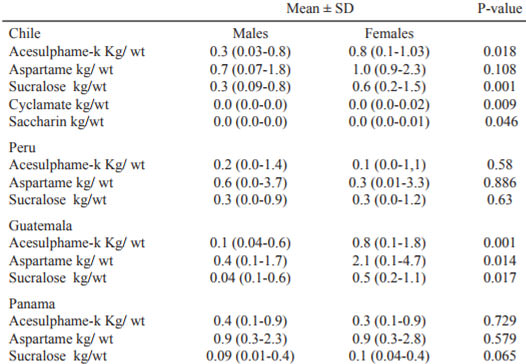
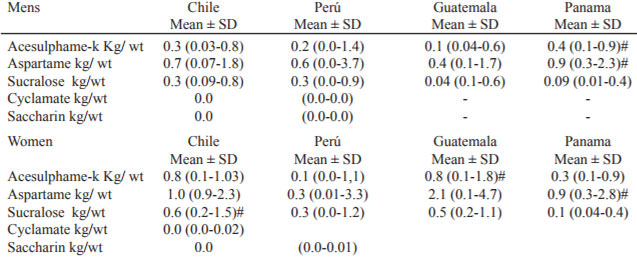
We found differences by sex and country only between Chile and Guatemala, with Chilean females consuming the most acesulphame-k, sucralose, and cyclamate (p<0.05) and Guatemalan females consumed more aspartame, acesulphame-k and sucralose (p<0.05).
We found no significant correlation among males in Chile and Panama between consumption (per kilo of weight) and BMI. Among males in Peru and Guatemala, however, consumption of aspartame and acesulphame-k and BMI were negatively correlated. We found positive correlations among females in Peru, Chile and Guatemala between BMI and total consumption, consumption per kilo of weight of acesulphame-k, aspartame and cyclamate (only in Chile).
Acceptable daily intake of sucralose is between 0-15, 0-40 for aspartame, 0-7 for cyclamate, 0-5 of saccharin, 0-15 of acesulphame-k and (11). For acesulfame-k, no student surpassed this amount, with the highest consumption being 58.7% of acceptable daily intake. Consumption of cyclamate beyond daily acceptable intake levels was reported by 1 Chilean student and 2 Chileans reported consuming above acceptable levels of sucralose.
The intake of artificial sweeteners has greatly increased across Latin America, as was shown in our study and other research conducted in Latin America. Among a sample children and adolescents in Chile report that 99.6% of elementary school children sampled ate food with artificial sweeteners (9), attributed mostly to consumption of zero calorie, inexpensive, carbonated drinks, whereas a multicenter study which was carried out on Latin American University Students which evaluated the intake of sugarless beverages showed that 80% of the students consumed at least 1 cup of a beverage without sugar per day (10).
In a study conducted among Brazilian adults, Zanini et al (11) found 22.7% of females and 13.9% of males ate foods with non-nutritive sweeteners. A study conducted in the U.S. that used the National Health and Nutrition Examination Survey (NHANES) (12), found that 15% of the population consumed artificial sweeteners present in food and drinks. It is important to mention that comparisons between countries should be evaluated with caution because of differences in methods, instruments used, study populations and time period evaluated.
The high levels of artificial sweeteners consumed in our study can be attributed to the intake of carbonated beverages, juices (readymade and powder forms), and sweetened milk products (i.e. flavour yogurt).
Artificial sweeteners are typically used as a nutritional aid to those who need to reduce their consumption of sugar or calories or need to manage their weight (13). Our differing results for men and women related to BMI and consumption of artificial sweetener is important to highlight, where BMI was positively related to sweetener intake in women, but not men. This may be related to advertisement that focuses primarily on the female consumer. Higher education level is also related to higher artificial sweetener intake, which may be related to an increased concern among persons of higher education levels to maintain a healthy weight. Another explanation may be that foods containing nonnutritive sweeteners (light or diet foods) are considered healthy products and that persons with greater education have higher access to these foods which are generally more expensive.
Among the surveyed countries, Chile was the only one in which cyclamate and saccharin were consumed on a daily basis. Very little was consumed or these particular sweeteners are not available in the other countries surveyed. There is a tendency to replace cyclamate and saccharin for other no nutritive sweeteners (9) included sucralose, aspartame, acesulfame-k and stevia (natural sweetener), possibly because of studies conducted in animal models showing an increased risk of bladder cancer (14) indicating that cyclamate and saccharin may negatively affect health. The role of artificial sweeteners in cancer risk has been widely debated since 1970, when researchers found an increased risk of bladder cancer among rodents given extremely high doses of saccharin (14). Later epidemiological studies also found increased risk among humans (14), although more recent studies do not find such association (15). Boselli and colleagues (16), for example, found no association between consumption of saccharin and risk of mouth, pharynx, oesophagus, larynx, breast, colon, rectal, kidney, ovarian, or prostate cancer. Later is was shown that the carcigenic effect of saccharin was specific to certain species (17). Despite these findings, consumer groups are against the use of saccharin and especially cyclamate in food products.
Traditionally it is thought that substituting artificial sweeteners for sugar can be an effective strategy to control weight, although findings are mixed (13). A modelling study recently published shows that a decrease of 40% of free sugars added to sweetened beverages for more than 5 years would result in an average reduction in energy consumption of 38.4 kcal per day (95% CI: 36.3-40.7) at the end of the fifth year. This would lead to an average reduction of 1.20 kg (1.12 - 1 .28) in steady-state body weight in adults, which would result in a decrease of 1.0 percent(from 35.5% to 34.5%) in overweight and 2.1 percent in obesity (from 27.8% to 25.7%) (18).
That artificial sweeteners do not satisfy appetite as well as sugar does is another issue under debate. It is even suggested that artificial sweeteners stimulate hunger and activate pleasure receptors, leading to eating in excess and an addiction to sweet foods (19).
Recent findings demonstrate an increase in the expression of transporters utilized in the intestinal absorption of glucose (SGLT1) and the induction and translocation of glucose transporters (GLUT2) in the membrane border when consuming artificial sweeteners. The increase of these changes could facilitate absorption and metabolism of ingested sugars (20). In the case of consumption of artificial sweeteners, however, since these changes are not accompanied by sugar intake, they may increase energy consumption. Additionally, a recent study has shown changes in the microbiota when consuming sweeteners. This is the case with a consumption equivalent to the IDA, favoring glucose intolerance (21). However, other studies show inconsistent results (22).
Studies in humans have documented the activation of different neural pathways in the hypothalamus when caloric sweeteners are consumed compared to artificial sweeteners, indicating that differences in sweeteners can be detected (23). Taken as a whole, these findings advance the hypothesis that the consumption of sweet, but non-caloric, foods produce significantly different effects compared to the consumption of sugar sweetened foods. These effects could, over time, contribute to a positive energy balance and an increase in body weight.
It is important that artificial sweeteners—the amount of each sweetner per serving size and for each 100 g or mls of prepared food—be listed on nutritional labels. Additionally, the daily recommended amount in mg/kg of body weight per WHO/FAO recommendations should also be noted.
The consumption of artificial sweeteners may be increased in Latin America, due to an increment in taxes on sugary drinks as is currently happening in Mexico, Ecuador and Chile as well as the new food labeling standards for foods high in sugars and other nutrients associated to health risks, conducted in Chile, which has lead to the change from sugar to artificial sweeteners in food and beverages by the food industry.
Within the limitations is possible to name the sample y not aleatory and is a transversal study, in no possibility to name of causality only association. It is neither possible to realize sensibility and specificity analysis of the survey, and can mention this the a low sample of men, since in general the majority of the students was of the area of the health. The strength we can is a first study in different countries in Latin America, use a validate food survey and in not a secondary data.
The current study demonstrated heterogeneous behaviour among the countries surveyed. Overall we observed high consumption of artificial sweeteners, especially among females. We also found that increased BMI was related to increase consumption among females, with the opposite being true in males. And finally, findings indicate consumption of artificial sweeteners within the daily recommended levels according to WHO/FAO standards. New products that contain artificial sweeteners arrive to markets daily, making the task of monitoring appropriate levels of consumption of these sweeteners difficult.
Recibido: 26-01-2017
Aceptado: 04-08-2017