
The study aims at understanding the role of early exposure to ethanol during childhood, in particular in the form of alcohol used in food preparation. A matched case control study was conducted in Italy and Germany. 300 cases were selected from the lists of the Alcoholics Anonymous Associations and 300 controls were matched from the general population. A CATI system was used for collecting information on drinking habits, family risk factors, age at first ethanol consumption, binge drinking episodes and alcohol ingestion as a food ingredient during childhood. Association of variables with the status of case were analysed using a multivariable conditional logistic regression. In the multivariable model four variables were selected: education, father drinking status, age at first ethanol consumption and binge drinking during adolescence. Consumption of food containing alcohol in common recipes was not associated with an increased risk of alcoholism in older ages. Drinkers having their first contact directly with alcoholic beverage before age 13 were more likely to suffer from alcohol dependence at some time during their life. On the contrary, using alcohol in food preparation during childhood does not appear to be related with subsequent risk for alcohol abuse.
Key words: Paediatric alcohol exposure; alcohol in food preparation; binge drinking
El estudio tiene como objetivo comprender el papel de la exposición temprana al etanol durante la infancia, en particular, la forma en la que se utiliza el alcohol en la preparación de alimentos. Este estudio de emparejamiento de casos y controles se llevó a cabo en Italia y Alemania. Se seleccionaron 300 casos de las listas de las Asociaciones de Alcohólicos Anónimos y se los emparejó con 300 controles obtenidos de la población general. Se utilizó el sistema CATI para la recolección de información sobre hábitos de consumo, factores de riesgo de la familia, edad del primer consumo de etanol, episodios de consumo excesivo de alcohol, e ingesta de alcohol como ingrediente alimentario durante la infancia. Se analizó la asociación de las variables con la situación de cada caso mediante una regresión logística condicional multivariable. En el modelo multivariable se seleccionaron cuatro factores: educación, relación del padre con el alcohol, edad del primer consumo de etanol y episodios de consumo excesivo de alcohol durante la adolescencia. El consumo de alimentos que contienen alcohol en las recetas comunes no se asoció con un mayor riesgo de alcoholismo en edades más avanzadas. Aquellos bebedores que han tenido su primer contacto directo con bebidas alcohólicas antes de los 13 años eran más propensos a sufrir de dependencia al alcohol en algún momento de su vida. Por el contrario, el uso de alcohol en la preparación de alimentos durante la infancia no parece estar relacionado con un riesgo posterior de abuso en el consumo de alcohol.
Palabras clave: Exposición al alcohol en edad pediátrica; alcohol en la preparación de alimentos; consumo excesivo de alcohol
Unit of Biostatistics, Epidemiology and Public Health, Department of Cardiac, Thoracic and Vascular Sciences, University of Padova, Italy. ZETA Research Ltd, Trieste, Italy. Prochild ONLUS, Trieste, Italy. Research Unit INSIDE, University of Luxembourg, Esch-sur-Alzette, Luxembourg.
The Alcohol use usually begins in the second decade of life, typically in early adolescence, when youths frequently adopt a binge-like drinking pattern (1): for the majority this behaviour may signify nothing more than a transient phase of experimenting with a risk behaviour, and many drinkers reduce their consumption in early adulthood (2). On the other hand, epidemiological data have shown that a potentially powerful predictor of progression to alcohol-related harm is age at first use, with studies suggesting that the earlier the age at which young people take their first drink of alcohol, the greater the risk of abusive consumption and the development of serious problems, including alcohol disorders (2).
Cross sectional (2) and longitudinal studies (3-6) investigating the relationship between early alcohol assumption and adult drinking pattern have mainly focused on alcohol use in adolescence, while little attention has been dedicated to the effects of alcohol exposure in childhood in determining later ethanol use and in developing alcohol use disorders (6). Moreover, exposure to alcohol during childhood seems to be a multilevel phenomenon including a wide spectrum of behaviours, such as using alcohol in food, or sipping or tasting others’ alcoholic beverages (7). The prevalence of such behaviours can be expected to be high among children; however, the developmental process through which children’s attitudes toward alcohol evolve in patterns of alcohol consumption during adulthood are largely unexplored and relatively little is known about this transition (8). The role played by the early exposure to alcohol in children due to food preparation is unclear and not well studied.
The aim of this case control study was to identify factors within family, childhood and adolescence which differente individuals experiencing hazardous and harmful alcohol use in adulthood from those who never experienced alcohol-related problems, with a particular focus on the role of exposure to ethanol during childhood and its use in food preparations.
For the purpose of the study, cases were defined as individuals with a lifetime history of alcohol-related problems, having experienced alcohol abuse in the past or still currently experiencing it as a significant problem. Therefore, cases were selected from the lists of the Alcoholics Anonymous Associations operating in the North-East of Italy (Veneto and Friuli-Venezia Giulia regions) and in South-Germany (Bavaria) which adhered to the study.
Controls were randomly selected from the population of the same regions using a Computer Assisted Telephone Interview (CATI) system. In order to correctly identify controls (people who had never experienced alcohol related problems), respondents were screened for lifetime alcohol related problems by means of the CAGE questionnaire (9). Written informed consent was obtained from all participants prior to taking part in the investigation. Data were treated according to the Italian law of Privacy Protection (Lex. N. 196/2003).
The study was designed to identify an OR of 1.6 or greater for the “alcohol in food consumption”, with an alpha level of 0.05 and a power of 0.80 in a 1:1 case-control study. We assumed an overall percentage of alcohol in food consumers of 30% of the total sample. In this scenario, a sample size of 596 subjects is needed, rounded up to 600.
Therefore, using the above mentioned procedure, 300 cases (150 Italians and 150 Germans) and 300 controls matched by age and sex were identified and underwent a faceto-face interview.
Cases and controls were interviewed individually by expert psychologists whose mother language was Italian or German (as appropriate depending on the sample) using a semi-structured interview. The interview aimed at extracting the information on all factors relevant for the purposes of the study including socio-demographic characteristics, health related indulgence behaviours (smoking), current drinking habits (drinking quantity and frequency and reasons, if any, for heavy drinking), family risk factors (relative’s drinking status), age starting alcohol consumption (including sipping or tasting others’ drinks), alcohol ingestion during childhood as a food ingredient, and ethanol consumption during adolescence (frequency of binge drinking episodes). All interviews were digitally recorded. For the purpose of this study, the rich qualitative data collected during the interviews had to be converted into categories of variables. This process is known as quantification, by which qualitative data are treated with quantitative techniques to transform them into quantitative data(10). Therefore, on the basis of the structure adopted for the interviews, two psychologists made an observation recording sheet allowing for the extraction of information on participants’ behaviours. The psychologists compiled the sheet independently, listening to the answers provided by the people during the interviews. The overall agreement between them in providing such dietary indications was very high, obtaining a Cohen’s Kappa of 0.74. A consensus was thus obtained for all discrepant interviews under the coordination of the datamanager of the project.
In order to define participants’ current drinking status, three substance use groups were derived from participants’ responses: current drinkers, former drinkers (abstainers in the past 12 months) and non-drinkers. For current drinkers, the interview plan was aimed to investigate the (a) drinking frequency (number of drinking occasions per time unit) during past year and (b) the quantity (litres) of alcoholic beverage (wine, beer, spirit) per occasion. Information from (a) and (b) were used to construct a measure of weekly alcohol beverages consumption; therefore, the number of standard drinks per week was calculated and current drinkers were classified into 2 categories: moderate and heavy drinkers.
Criteria for heavy drinking were based on low-risk drinking guidelines for adults ≤65 from the National Institute on Alcohol Abuse and Alcoholism (NIAAA): daily limits of ≤4 drinks for men and ≤3 drinks for women, and weekly limits of ≤14 drinks for men, ≤7 drinks for women(11). All other respondents that declared to not exceed these limits were considered moderate drinkers. The frequency of binge drinking episodes at present and during adolescence was also investigated, with binge drinking being defined as consuming 5 or more US standard drinks (male) or 4 or more drinks (female) within approximately 2 hours. Parents’ drinking habits were also evaluated adopting these definitions.
Finally, childhood exposure to alcohol was explored asking information about the age at first tasting (including direct tasting alcohol and consuming alcohol in food), frequency of ingestion of alcohol as a food ingredient and details regarding the type of food (meals or sweets) and the alcoholic beverages tasted in food.
Being a non-intervention survey, no formal evaluation by an Ethical Committee is needed in Italy. Written informed consent was obtained from all participants prior to taking part in the investigation. Data were treated according to the Italian law of Privacy Protection (Lex. N. 196/2003).
Distribution of the main socio-demographic characteristics and health related indulgence behaviours were compared in case and control, and drinking habits of both groups were described. Distribution of factors usually considered as developmental determinants including parents’ drinking status and alcohol exposure during adolescence were assessed. Moreover, differences in exposure to alcohol during paediatric age were also evaluated. Continuous variables were always expressed as median and inter-quartile difference and categorical variables as percentages and absolute numbers. Differences between groups were compared using Wilcoxon and Chi-Square Fisher test, as appropriate.
Association of variables with the status of case was investigated using a multivariate conditional logistic regression model, matched by age and gender.
All variables considered were entered into the model “as is”, i.e. without any transformation or cut-off. If significant non-linearity using a score test was present, in relating the covariate’s effect with survival, the specific covariate’s effect was modelled using a restricted cubic spline. Selection criteria was the AIC (Akaike Information Criterion) applied backward for selecting significant covariates. The final model for each of the three steps was selected if superior in terms of AIC at a significance level of 0.05 and p-values were explicitly indicated if below the 0.25 threshold, otherwise the “NS” indication was used.
To account for possible overfitting in the regression model secondary to high ratio between covariates and events, cross-validation and bootstrap (2000 runs) techniques were applied. For the logistic regression model, Somer’s concordance Index Dxy (the closer to one in absolute value, the better) was obtained and evaluated for this purpose.
Multivariate Odds Ratios are presented along with their 95% confidence intervals.
The statistical significance was settled at p <0.05. The R System (release 2.7.0) statistical package and the Harrell’s Design and Hmisc libraries were used for analysis.
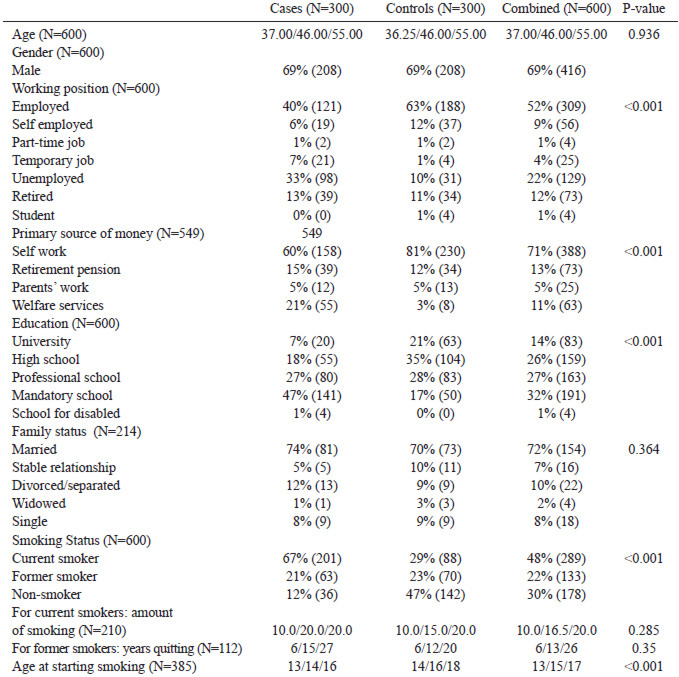
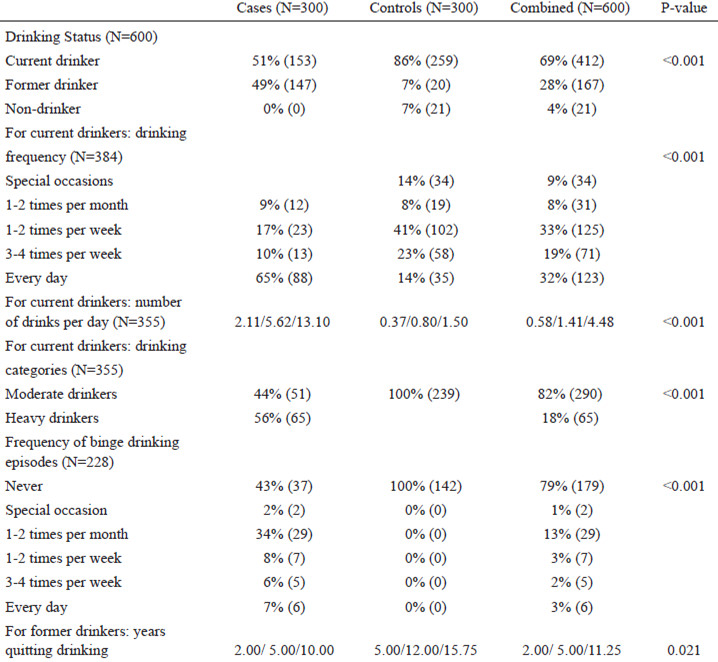
Socio-demographic characteristics and health related indulgence behaviours of cases and controls are shown in Table 1. There are significant differences regarding education, working position, and the primary sources of income, with cases having less frequently reached higher education level and being more frequently unemployed. Moreover, smoking habits are more diffuse among cases, with the latter having started to smoke at a younger age than controls. Current drinking habits are described in Table 2. Fifty-six percent of cases reported to still being heavy drinkers. Among the reasons for heavy drinking, participants pointed out social reasons (31%), work and economic reasons (19%), pleasure (14%) and family problems (9%).
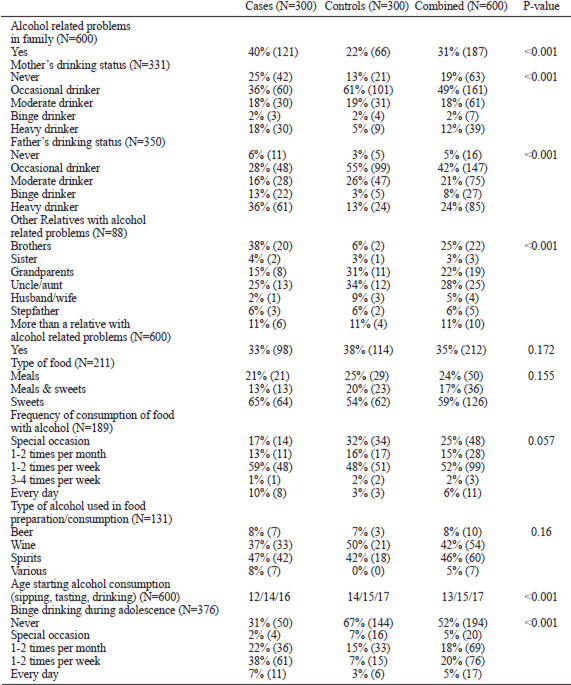
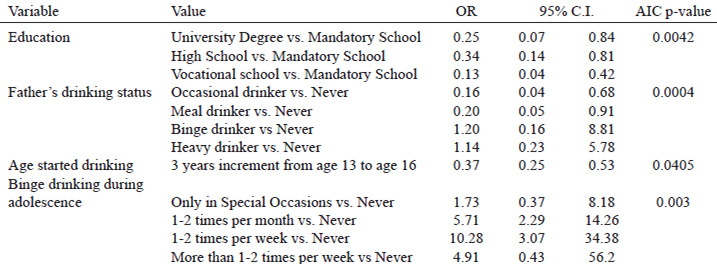
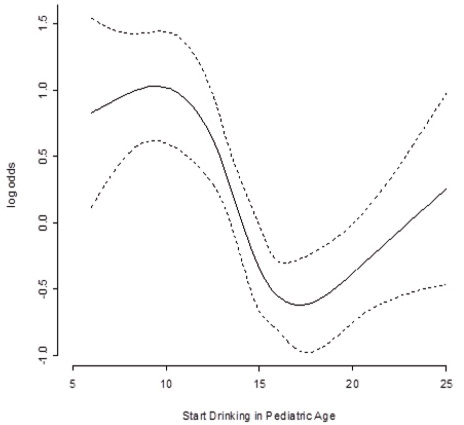
The distribution of developmental risk factors in cases and controls is shown in Table 3. Having a problem drinker among relatives is strongly associated with the status of case; similarly, a lifetime history of alcohol-related problems is predicted by early experiences with alcohol consumption (including sipping and tasting others’ drinks) and by higher frequency of binge drinking episodes during adolescence. As opposed to the latter finding, consuming alcohol in foods during childhood is not related to subsequent risk to engage in problem drinking. In multivariable analysis (Table 4) the final model selected four variables: education, father drinking status, age starting drinking, tasting or sipping alcohol and binge drinking during adolescence. More specifically, a U-shaped association between alcohol drinking, tasting, sipping debut and alcohol abuse during adult age emerged, declining from age 13 to 16 years (OR 0.37 95% CI 0.25- 0.53) and increasing again in late adolescence (OR 3.31 95% CI 1.08-10.17) (Figure 1).
The consumption of alcohol is a socially accepted “norm” in most populations in western societies, with most individuals beginning to drink in their mid-teens (12). This behavioural pattern is similar for boys and girls and consistent across countries (13). Most of the studies agree that during the mid-teens the probability of drinking increases rapidly with each year beyond age 12, especially in cross-sectional and prospective evaluations rather than retrospective histories (12, 14).
Early experimentation with alcohol makes adolescence a critical period for the onset and increase of alcohol consumption. Problem drinking during adolescence is a public health issue not only because of the immediate consequences (e.g., road traffic accidents, contribution to other intentional or unintentional injuries, high-risk sexual behaviour, comorbid substance use, academic problems) but also because early drinking may lead to long-term alcohol problems (12). Particularly, adolescent binge drinking seem to be a highrisk behaviour associated with significant later adversity including a higher risk of adult alcohol dependence/abuse as pointed out in previous studies and confirmed in the present case control study (15).
During the past two decades, a burgeoning literature has emerged establishing an association between age of drinking onset and risk for later hazardous alcohol consumption and dependence. Both cross-sectional (16-18) and longitudinal studies (19, 20) have indicated that the age at drinking onset is one of the strongest predictors for the development of later alcoholrelated problems. Moreover, early onset also predicts tobacco and other drug involvement, psychopathology, poor academic achievement, unintentional injury, violence, and suicidality (21, 22).
Nevertheless, although frequently described, the mechanisms underlying the relationship between age at first drink and subsequent alcohol related problems remain unclear, with some studies finding age at first drink to be only a weak predictor of heavy drinking in adolescence (23, 24) or in later life (25).
The effects of alcohol consumption in preadolescence remain largely under-explored. In a longitudinal study only Fergusson et al.(26) focused on the relationship between childhood alcohol consumption and adolescent drinking patterns evaluated at 15 years of age. This study used a birth cohort of 739 children, and extensively investigated the effects of early exposure to alcohol. Age at first alcohol consumption was classified into four categories: 0 to 5 years, 6 to 10 years, 11 to 12 years, and after 13 years. The authors point out that children who had been introduced to alcohol before the age of 6 years were 1.9 to 2.4 times more likely to report frequent, heavy or problem drinking at age 15 years than children who did not drink alcohol before the age of 13.
In this retrospective study, we investigated the risk of alcoholism according to the age at which individuals started consuming alcohol, finding a non-linear effect: the risk in fact declines from 13 to 16 years (OR 0.37 95% CI 0.25- 0.53) of age and then increases up to 25 years of age thereafter (OR 3.31 95% CI 1.08-10.17).
These results are consistent with those reported in a study by Pape (27), which explored how age at first intoxication with alcohol relates to mental health, social integration and adjustment to adult role. A U-shaped association between intoxication debut and psychological problems arose among males, implying that not only early but also late beginners had more such problems than those who had followed the mainstream. In particular, male late beginners were psychologically healthy, but they showed indications of a delayed entry into the adult role. The authors concluded that getting drunk for the first time in mid-adolescence seems to be a phenomenon in the normal development of young males.
Heavy alcohol consumption and associated problems may also be affected by a variety of factors other than age at first alcohol experience. One such domain relates to genetic factors as measured through a family history of alcoholism, which, while contributing most robustly to heavier drinking, alcohol problems, and alcohol use disorders (17), may also impact on the decision to drink (28). A related issue that might enhance drinking behaviour involves the home environment(12). Among younger adolescents, observing drinking at home, especially by their parents, can have an important impact on a person’s decision to drink (12). Moreover, developmental studies demonstrate that the emotional context that accompanies parental use of ethanol has a profound effect on how young children (3 to 6 years) judge the pleasantness of the smell of an ethanol beverage, similar to what occurs with tobacco smoke (29). Children whose parents use ethanol primarily as a means of obtaining relief from their problems are more likely to consider the odour of beer as unpleasant than those whose parents drink for other reasons(30). Consistently with these observations, in our study, a lifetime history of alcohol-related problems seems to be strongly predicted by father drinking status.
Even if some studies testify that early childhood represents a “sensitive period” for the development of expectancies and cognitions about alcohol, and particularly that associative learning in the context of emotionally salient conditions is a powerful mechanism by which odours acquire personal significance, to our knowledge the present case control study is the first to expressly investigate the role of alcohol contained in food during childhood: interestingly, early familiarity with alcohol consumed in food, probably emotionally connected to family socialisation, seems not to be associated with later alcohol related problems.
Nevertheless, the present study shares the limitations of retrospective study designs, both in terms of inference and extrapolation from our results. Measures of behaviours and negative outcomes relied in fact on the honesty and accurate recollection of respondents (31). Studies have found that people can simultaneously hold conflicting conceptions and beliefs which may cause them to respond in seemingly contradictory or inconsistent ways (32). Additionally, poor or incomplete memory of events, external influences, and lack of time to fully recall information may lead to purposefully or accidentally inaccurate recall and responding. Also, some people may respond based on what they believe is socially desirable rather than what they think is true (32); problems related to data quality in terms of validity, accuracy, reliability and completeness (item non-response), have been largely discussed, mostly in terms of the accuracy of self-reports, in the studies evaluating alcohol consumption.
The method used in this study (i.e. semistructured interviews) was specifically chosen to minimize any bias which may have been potentially occured by forcing people to choose, in answering, from a predetermined set of options, therefore leaving the maximum freedom and complexity to each answer.
The work has been partially supported by an unrestricted grant from the Italian Ministry of Foreign Affairs under the programs “Programmi di alta rilevanza scientifica e tecnologica” Italia-Messico and Italia-Argentina, and from Prochild ONLUS (Italy).