
The objective of this study was to evaluate the relationship between dietary pattern and incidence of nutrition-related non-communicable diseases in Serbia, a country which has experienced a significant shift in nutrition and lifestyle habits, guided by its particular historical background and its rapid transition to liberal economy. Data was collected from annual reports published by the Statistical Office of the Republic of Serbia and the Institute of Public Health. It provides a focus on the timeframe of 1997-2014, in order to capture any changing pattern after the year 2000, in which the process of complete trade liberalization started.The results have shown a striking growing trend in both disease incidence on the one hand and processed food items such as processed meat, fruit juices, chocolate and biscuits and on the other hand. Granger causality test suggests that there exists causality that goes beyond spurious relationship between the disease of blood and blood-forming organs and immune system disorders and average per capita consumption of fruit and vegetables, poultry, processed meat, chocolates and biscuits and fruit juices. Also, we find evidence of long-term relationship between fish consumption and endocrine, metabolic and digestive diseases.
Key words: Food pattern, disease incidence, economy liberalization, processed food.
El objetivo de este estudio fue evaluar la relación entre los patrones de dieta y la incidencia de las enfermedades no transmisibles relacionadas con la nutrición en Serbia, un país que ha experimentado un cambio significativo en los hábitos de nutrición y estilo de vida, guiado por sus antecedentes históricos particulares y su rápida transición hacia una economía liberal. Se recogieron datos de los informes anuales publicados por la Oficina de Estadística de la República de Serbia y el Instituto de Salud Pública. Se hizo foco en el período de 1997 a 2014, con el fin de poder detectar cualquier cambio en los patrones a partir del año 2000, cuando comenzó el proceso de liberalización total del comercio. Los resultados han mostrado llamativamente una tendencia creciente tanto en la incidencia de enfermedades como en la proliferación de alimentos procesados, tales como carne procesada, jugos de frutas, chocolate y galletas. La prueba de causalidad de Granger sugiere que existe una relación de causalidad que va más allá de la relación espuria entre las enfermedades hematológicas, las afecciones de los órganos hematopoyéticos y del sistema inmunológico y el consumo promedio per cápita de frutas y hortalizas, productos avícolas, carne procesada, chocolates, galletas y jugos de frutas. Parece evidente también la existencia de una relación a largo plazo entre la aparición de enfermedades endocrinas, metabólicas y digestivas y el consumo de pescado.
Palabras clave: Patrones alimentarios, incidencia de la enfermedad, liberalización de la economía, alimentos procesados.
Faculty of Economics Subotica, University of Novi Sad (Serbia). Unit of Biostatistics, Epidemiology and Public Health, Department of Cardiac, Thoracic and Vascular Sciences, University of Padova (Italy). Department of Nutrition, University of Buenos Aires and Food and Diet Therapy Service, Acute General Hospital Juan A. Fernàndez, Buenos Aires, Argentina.
Nutritional pattern, commonly defined as a “Western diet”, is typically characterized by high intake of refined carbohydrates, added sugars, fats and animal-source foods on the one hand and low intake of legumes and coarse grains, on the other (1). It strongly influenced many traditional food and cuisine (1), and become a feature of modern dietary patterns in many low and middle-income countries (2). Food pattern modifications rose with new technology development and diffusion, income growth and retail globalization (1,3). Commercial interactions between nations affect food chain through leveraging the importance of import, allow a global spread of supermarkets (thanks to the Foreign Direct Investments) and contribute to evolution of preferences and cultural expectations of population via commercial promotion of food (4). New technologies, among other things, contributed to a worldwide increase in use of caloric sweeteners and vegetable oils such as soybean, sunflower, rapeseed, palm and groundnut oil (2–5). Individual intake of inexpensive vegetable oils increased threefold to six fold throughout the developing world (1). Furthermore, the increase in per-capita income, together with population growth and progressive urbanization is highly correlated with “livestock revolution”, resulting in an unprecedented growth in demand for food of animal origin in developing countries (6) as well as consumption of a more processed food (1,7). Retailing globalization, with an enormous impact on the market structure in transition and developing countries (8,9), provides access to many new empty calorie foods and beverages and reduces the intake of fresh food, which represents an important source of nutrition.
Different studies have discussed potential adverse effect of the penetration of transnational food and drink companies on public health in developing and developed countries (10, 11). A displacement of traditional food systems has the potential to undermine public health more in low and middle income countries than in high-income countries, which already industrialized their dietary patterns (3). The dietary changes are very rapid and most probably will continue to evolve without suitable policy intervention (12–15).
“Nutrition transition” occurs concomitantly with two remarkable processes: demographic transition and epidemiological transition related to urban-industrial lifestyles. This results in an increased prevalence of obesity and contributes to the incidence of chronic and degenerative diseases (2). Now, nutrition-related non-communicable diseases (NCDs), most particularly cardiovascular disease (CVD) and some types of cancer, replaced previously dominant transmissible diseases in low and middle income countries. CVDs constitute the largest cause of mortality, representing 31% of all global deaths in 2012 (16). Over three quarters of CVD deaths take place in low and middle income countries affecting a nation’s economic development through loss of income and the high cost of medical care (17).“Western diet” nutritional patterns,as well as frequent consumption of processed and ultra-processed food,promote obesity, metabolic syndrome, CVDs and, most probably, favor autoimmune diseases (18).
However, Serbia is a very particular case of middle-income country: it is one of the transition economies in Central and Southeastern Europe (CEEs), whose system rapidly switched from planned to market economy after the 1990’s. In pre-transitional era only a limited range of food items were available, but due to low food prices and significant state agriculture subsidies, the typical diet found in these countries had features of high-income diets: a significant consumption of livestock products (19). Since the grain production was highly subsidized, bread was often used to feed livestock in small farms (20). Also, public health expenditures (as a percentage of GDP), was significantly higher in socialist countries than in most middle-income countries (20).
The biggest hyperinflation after World War II that has hit Serbia in the 1990s, gray economy, civil war, an influx of about one million refugees, international economic sanction – are all factors that contributed halving the size of the Serbian economy with respect to the early 1990s. (21).
Despite severe economic difficulties, Serbia has preserved its strong agricultural basis as it has historically been an important agricultural producer for both domestic and export market (19). Furthermore, there is a strong culinary tradition and efforts to preserve traditional food products and food cuisine (22).
Taking into account abrupt changes which occurred upon opening of the borders for competitive import, reduction of agricultural subsidies and shrinking of value added in agriculture, deterioration of social safety nets, (20) it is no wonder that important changes were experienced in terms of prevalent dietary patterns. It is interesting to notice that the evolution in food consumption did not concern the expansion of food quantity in a measure in which it concerned the diversification of available food items (20).
It is believed that Serbian population has been heavily affected by wars, disintegration and political crisis, resulting in an increased mortality from cancer and ischemic heart disease during the past two decades (23, 24). Since the 1990s, NCDs have represented a major cause of death, where cardiovascular diseases are the top ranked, followed by cancers (25). Dietary risk, along with tobacco smoking and high blood pressure, account for the most of the disease burden (26). Aging population and high burden of NCD mortality resulted in a continuously increasing crude death rate, which reached 13.97% in 2008. According to the national health survey in 2006, 54.5% of adult population were overweight and 18% children aged 7–18 were at least moderately obese. Only 23% of adult population reported undertaking physical activity on daily basis, with 67% of adults being physically inactive (27).
The aim of this paper is to provide consistent evidence about the long term relationship between dietary pattern and incidence of NCDs, in a very particular setting of Serbia which has undergone one of the most unstable transition experience in the CEEs.
Our literature review did not show many articles interested in the in analyses of long-term relationship between dietary pattern and disease incidents (28–30) To the best of our knowledge, this study is the first to document a significant shift in dietary pattern, and addresses the relationship between food consumption and incidence of broad categories of non-communicable diseases
Time series data about average per-capita food consumption is taken from the Statistical Office of the Republic of Serbia (31). Yearly data on diagnosed disease incidence was taken from the Institute of Public Health of Serbia “Dr Milan Jovanovic Batut” (32). Diseases, conditions and injuries in primary health service, provided by state-owned primary health centers are presented in uniform lists in accordance with the International Classification of Diseases – 10th Revisions (33). We have analyzed four groups of diseases: diseases of the blood and bloodforming organs and certain disorders involving the immune mechanism (D50-D89), diseases of the circulatory system (I00-I99), endocrine, nutritional and metabolic diseases (E00-E90) and diseases of the digestive system (K00-K93) (Table 1).
We have selected relevant food categories that constitute a typical household diet, aggregating over certain food items. The categories are bread and paste products, fresh fruit and vegetables, milk products (fresh and fermented), red meat (beef, pork and goat), processed meat (dried bacon, dried meat boneless, dried meat with bones, salami and sausages all kinds, hot dogs, etc.), fish, poultry, fruit juices, processed snack food (sweets and biscuits) and total fat.
The data refers to the time frame of 1997-2014. We chose this period to evaluate the changes after the year 2000, the year of economy “opening”, which can be considered as the year when the process of complete trade liberalization started. The conclusion relates to the “opening” of the economy since 2000 relating to the completely closed economy until then. After parliamentary elections in December 2000, the EU lifts tariffs on import of goods from Federal Republic Yugoslavia (The Republics of Serbia and Montenegro together established a federation in 1992) and the prospect of a Stabilization and Association Process was settled, in accordance with decisions of the EU Council (34). This has exposed agricultural producers to the increasing international trade competition. Besides this, Serbia has the signed Central European Free Trade Agreement (CEFTA)- agreements on free trade with the CEFTA countries, as well as free trade agreements with Russia, Turkey and Belarus. As a consequence, the aggregate supply of agricultural and food products has exceeded the demand in the period after the 2000 (35).
Multivariate time series analysis was conducted using as a reference standard cointegration approach. Pearson correlation coefficient and generalized regression modeling were used as a starting point, to underline problem of spurious relationship between the time series. Dickey- Fuller test was used to confirm level non- stationarity of the series, which can be visualized through graphical inspection (see Figure 1 and Figure 2). The order of the integration was determined using Kwiatkowski–Phillips–Schmidt–Shin (KPSS) tests, where the null hypothesis was that an observable time series is trend stationary against the alternative of a unit root (36). Since we have found that most series are of order 1, we have used a bivariate multivariate time series approach to establish long run relationship between the food pattern and disease. In particular, Granger causality test was used determine whether the lagged dietary pattern provide statistically significant information about the current values of outcomes (37).
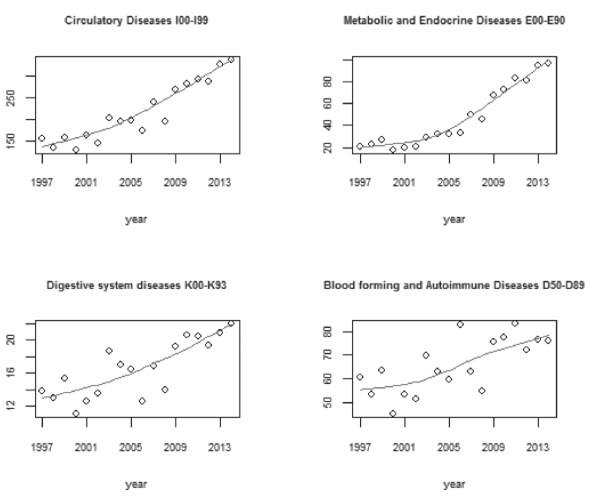
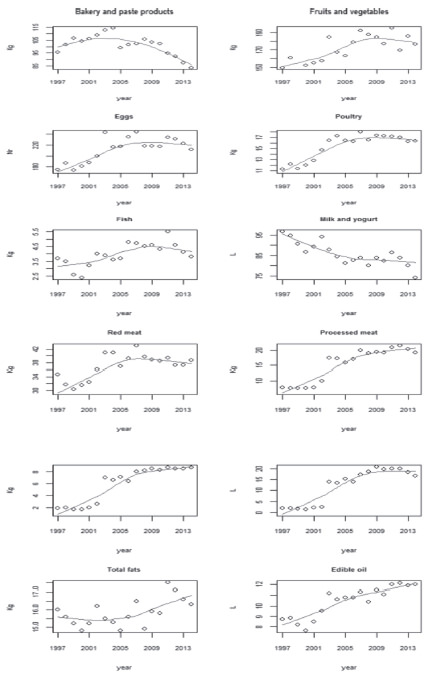
There is an evident growing trend in both disease incidence and food items such as processed meat, fruit juices and chocolate and biscuits in the observed period (see Figure 1 and Figure 2). Most notably, endocrine, nutritional and metabolic diseases (E00-E90) incidence rates have almost quintupled from 0.02 in 1997 to more than 0.09 in 2014. Circulatory diseases (I00-I99) have doubled from 0.15 to more than 0.30. Prevalence of blood forming and autoimmune diseases (D50-D89) and diseases of the digestive system (K00-K93) has also increased for 58% and 26%, respectively. In relation to food consumption, the highest growth can be observed in the consumption of fruit juices, and chocolate and biscuits, 9.3 and 6.6 times, respectively. Processed meat consumption has increased almost 2.5 times. Regarding fresh meat, the largest increase in total consumption is recorded for chicken (about 45%). The consumption of individual edible oil, fresh fruits and vegetables and total fish had also increased for 38%, 18%, and 32%, respectively. In the same period of time, consumption of fresh milk and yogurt has decreased by 23%. Similar declining trend can be noticed in consumption of bakery and paste products.
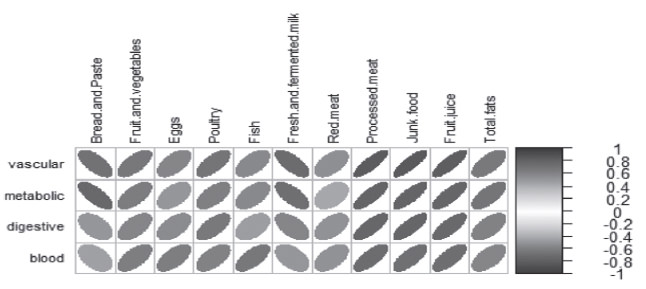
Preliminary descriptive (graphically represented Pearson coefficient) suggest that there is strong interdependency between the dietary patterns and the annual incidence of non-communicable diseases (see Figure 3). Bread and paste products and milk products and fermented derivatives seem to have a risk-protective relationship with all the four disease groups. Fruit juices, processed snack good (defined as sweets and biscuits) and processed meat seems to be strongly positively correlated with the disease incidence.However, since unit root test confirms that the series are not stationary, the assumptions behind standard linear modeling can be violated, hence the correlations shown in Figure 3 might be misleading.
In order to investigate the nature of stationarity of the series, we have performed KPSS tests on each series (see Table 2). Nonsignificant p-value (with p>0.05) means that the series is stationary around a deterministic (increasing or decreasing) trend. The lag order refers to the order of integration of the series.
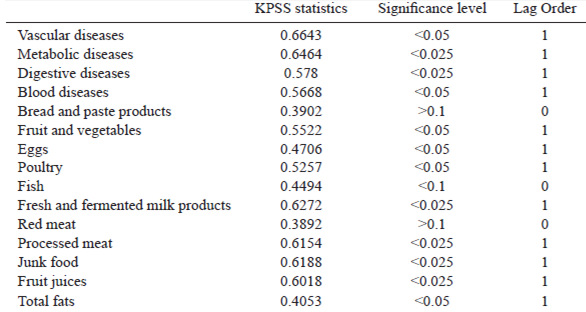
What we find is that, among all, only several time series (bread and pastry products, fish and red meat) are trend stationary. This means that they remain stable around the deterministic trend and are hardly influenced by external shocks. All other series are “shock sensitive”, meaning that any external shock (an event that has impact on the time series) permanently affects the series. In each case (trend stationary or integrated time series), standard assumptions for linear modeling fail, hence an alternative approach for testing the association between the dietary pattern and disease incidence is necessary.
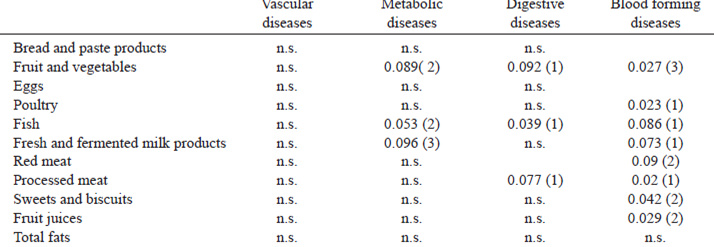
Table 3 presents a more rigorous statistical testing using Granger causality test for long run relationship between the variables. Significant p-value means that the past values of the independent variable (diet) are significant in predicting dependent variable (disease) up to the lag indicated in the brackets. This test suggests that there exists causality between the disease of blood and blood-forming organs and certain disorders involving the immune mechanism (D50-D89) and average consumption of fruit and vegetables (p= 0.03), poultry (p=0.02), processed meat (p=0.02) sweets and biscuits (p=0.04) and fruit juices (p=0.03). The same test suggests causality between both endocrine, nutritional and metabolic diseases (E00-E90) and diseases of the digestive system (K00-K93) (p=0.05 and p=0.04, respectively) and fish consumption. We found no significant relation between diseases of the circulatory system (I00-I99) and specified food items.
Road border changes, wars, coexistence of different nations resulted in very heterogeneous cuisine. Traditional Serbian cuisine is based on Slavic traditions with strong Mediterranean (Byzantine/Greek), Oriental (Turkish) and Hungarian influences (38). Many food items such as relish from bell peppers or eggplant, jams, jellies, pickled food, sausages, clotted cream, yogurts, syrupy fruit conserve as well as fruit brandy are homemade. The Serbian diet is traditionally heavy on grilled meat, sausages, local cheeses and bread. There are a number of local dishes which highlight this, such as pljeskavica (mixture of lamb or pork and beef, grilled with onions and served hot on fresh bread) and rostilj (various unseasoned grilled meat and can include chicken wrapped in bacon and stuffed with cheese). In recent years, bakeries can be found everywhere in Serbia and cater to the food to go aspect of life (39).
After the Second World War, new Yugoslavian agricultural policy (development of social farms, new approach to cooperatives, stimulation of personal labor, price investments) has resulted in a very rapid growth of agricultural production. In the period 1957-1980 the group activities, directly dependent on the production of raw materials have recorded extremely rapid development. The food industry (meat, fruit and vegetables processing as well as milk preserving and drink production) overshadowed the food processing in households. Rapid supply growth was registered for bread grains, fats, fruits, sugar, ready to eat meals and drink (40). The share of the agricultural population, total and active, decreased in the period 1948 -1980 from 67 or 73% to only 29 or 38% (41). These very fast socio-economic changes in Yugoslavia had a significant impact on food patterns causing consumption growth of finished and semi-finished products(38).
After a period of economic and political uncertainty (1990-2000) Serbia started new era of “democratic changes”, the process of complete trade liberalization started, the growth of GDP began and urbanization brought changes in lifestyle. All these elements resulted in changes in food habits of the population. One theory states that a key constituent is penetration of modern supermarkets (42). After the privatization of the retail sector and the establishing of the first supermarket chains, this region faced an inflow of foreign supermarket chains: Belgian Delhaize Group, German Metro Group, French Intermarché, Slovenian Mercator and the Croatian Agrokor. Slovenian chain Mercator as well as Veropulus Super Market Group (Super Vero) opened its first hypermarket in Belgrade in 2002. Intermarché has been present in Serbia through local brand Interex since 2004 when it opened its first supermarket. Idea (Agrokor Group) and Metro Cash&Carry are retails chain with a constant market share growth since 2005, when the first store was opened in Belgrade.
Socio-economic conditions and population health are inextricably linked, and strongly interdependent(32) and Serbia has been a rather good example to confirm this theory. In parallel with ‘westernization’ process of food habits (43) Serbia has experienced the general deterioration of public health (44). Adulthood obesity prevalence forecasts (2010–2030) predict that in 2020, 44% of men and 31% of women will be obese (45). Top three causes of death in the period 2000-2012 were CVDs: stroke, cardiomyopathy- myocarditis and ischaemic heart disease (31,46). One study has shown the markedly increasing trends in mortality rates from ischemic heart disease in man during 1991-2010 periods (30).
Disease yearly incidence rate trend graphs (Figure 1) show some striking evidence about the increase in all the considered groups of diseases. While circulatory diseases incidence rates have doubled, metabolic and endocrine diseases have almost quintupled. Even digestive and blood forming and immune diseases show an upward trend, although less systematic and more disperse around the mean.
The evolution of cardiovascular disease trends in Serbia is in line with several eastern European countries, notably Russian federation, where CVDs mortality remains high (47). Trends regarding endocrine, metabolic and nutritional diseases are coherent with trends in many countries, especially if we consider overweight, obesity and diabetes which become a global health challenge (48).
Like in the developing world, where diets are shifting rapidly and going to high consumption of fat, sweets, animal source food and processed food (2,14), similar trend is observed in Serbia. The evolution of dietary patterns in general is also in accordance with Mediterranean countries, such as Greece where consumption of animal fats and high-calorie foods is increasing(49).
In the 18 period time frames it appears that the Serbian population has evolved its preferences (on average) towards certain food items: there is an important increase in consumption of poultry, processed meat, chocolate and biscuits, fruit juices and edible oils. This means that despite the efforts to preserve culinary heritage (majority of consumers eat at home and like cooking) and traditional food as a response to modernization processes (22,50) Serbia did not resist changes that are happening in the rest of the world. From 2002 to 2003 there has been a structural break, driven by opening new hypermarket stores (Mercator, Super Vero and Univerexport) in 2002 and huge increase in per capita gross national income (GNI) from USD 1.590 in 2002 to USD 2.130 in 2003 (51). This has fostered a significant shift in consumption of these goods, and can be observed in our data (see Figure 2). Upward trends are present, although less striking, in red meat, fish, eggs and fruit and vegetable consumption. On the contrary, downward trend brought milk products from 95 l per capita to 75 l per capita. Similar trend occurred in bakery and paste products consumption.
Since the dietary pattern and disease incidence rate move together in parallel, descriptive evidence does suggest that there is strong relationship between the consumption of certain food items and disease insurgence. However, claiming causality in these type of studies is overly ambitious tasks, especially for the fact that in the multivariate time series context, testing for linear relationship between the variables might lead to erroneous results due to spurious relationship problem. However, long-term causality test has confirmed causality between the certain diseases, especially blood forming diseases, and a range of food items (processed meat, junk food, fruit and vegetable, etc.). However, these results should be interpreted overall, as a descriptive evidence of a trend in dietary pattern which had both strong trend and structural break and lead to non-ignorable consequences in disease incidence.
Most probably, dietary modifications should form the ground for action for all four group diseases prevention. To find ways to push people to change their dietary habits into more a healthy diet is the challenge for coming years for national competent authorities (52). This going to be particularly difficult in Serbia since there is an insufficient involvement of the state regarding adoption of national dietary guidelines (53).
National statistical data provides striking evidence about the ”Nutrition transition”, in particular the shift in consumption of processed food items such as processed meat, fruit juices, chocolate and biscuits. Our results indicate that this dietary transition represents one strong potential driver of chronic conditions. The analysis shows strong evidence of correlation between consumption of certain food items and blood forming disease, although a more detailed data would probably allow for a clearer identification of causal patterns and long-run interactions.
Although this represents a rather descriptive study of a very complex phenomena, to the extent of our knowledge, it is the first study to address the issue of long-term associations between the shift in diet orientation and chronical conditions in Serbia. As described, Serbia represents a very unusual context where it would be particularly relevant to broaden the knowledge in the field of nutrition-related morbidity. Lack of consistant academic programs in nutrition and national dietary guidelines represent important obstacles to building an efficient food and health system, which would ensure strengthening the population resilience to nutritional risks.
Monitoring of the situation is extremely important, since it represents the stepping stone for evidence-based action, necessary to tackle the burden in terms of public health cost. Longitudinal country-level data allows for general monitoring of the evolution of dietary habits and disease epidemiology, however only individual level data would allow for further inspection of the mechanisms through which policy action and nutrition yields health effects.