
 ,
Louise Rodrigues2 ,
Carlos Ramos-Urrea3
,
Louise Rodrigues2 ,
Carlos Ramos-Urrea3
No systematic reviews had analyzedthe most effective training for adolescents with obesity, thus, the aim of our review was to understand whether aerobic, resistance, or combinate, is appropriate for improving body composition, and factors associated with obesity in adolescents. We followed PRISMA methods, in the Pubmed, SCOPUS, and Web of Science databases, using the terms Obesity, teenager, fat mass, body mass index, body mass, intervention, aerobic, resistance, training and physical activity. Subsequently, titles and abstracts were read to filter the articles. Of the 3585 results found, 10 articles were selected with protocols of 3 to 4 weekly training sessions of 15 to 60 minutes, with interventions of 4 to 12 weeks. All types of training were beneficial for anthropometric and biochemical improvement, only resistance training (RT) has a significant difference for muscle mass compared to aerobic training (AT). Even though of the small number of studies with this type of comparison, it is still unclear which type of training is better or whether the two done concurrently would be a better alternative. According to our findings adolescents who want to maximize the effect of exercise on anthropometric variables should ideally perform aerobic and endurance exercises, but significant benefit can be achieved through any type of exercise, and if it were to have a significant differentiation within muscle mass the resistance exercise may be ideal to achieve this goal. Arch Latinoam Nutr 2020; 70(4): 290-299.
Key words: Exercise, obesity, adolescents, intervention.
En este artículo de revisión, fue analizado cual es el método de entrenamiento que es más efectivo para adolescentes con obesidad, de allí, a que nuestro objetivo en esta revisión es definir cual de los protocolos de entrenamiento (aeróbico, de resistenciao combinado) es mas apropiado para mejorar la composición corporal y otros factores asociados con la obesidad en adolescentes. Siguiendo los métodos de PRISMA se realizóla búsqueda en las bases de datos de, Pubmed, SCOPUS, y Web os Science, utilizando términos de obesidad, adolescentes, masa grasa, índice de masa corporal, masa corporal, intervención, ejercicio aeróbico, ejercicio de resistencia, ejercicio combinado y actividad física, subsecuentemente se leyeron títulos y resúmenes para filtrar los artículos. De los 3585 artículos encontrados, 10 artículos fueron seleccionados con protocolos de 3 a 4 días a la semana, donde cada sesión era de 15 a 60 minutos, con intervenciones entre 4 y 12 semanas. Todos los tipos de entrenamiento fueron beneficiosos para mejorar composición corporal y parámetros bioquímicos, el ejercicio de resistencia demuestra tener diferencia con relación a los otros dos protocolos de entrenamiento donde post-intervención consiguen mejorar la masa muscular. Debido al número pequeño de estudios aun la información es poco clara sobre cual protocolo es más efectivo y así poder elegir una alternativa mas adecuada. De acuerdo con los hallazgos realizar ejercicios aeróbicos y/o combinados mejoran la composición corporal a nivel de masa grasa, y el ejerciciode resistenciademuestra mejorar musculatura en adolescentes con obesidad. Arch Latinoam Nutr 2020; 70(4): 290-299.
Palabras clave: Ejercicio, obesidad, adolescentes, intervención.
https://doi.org/10.37527/2020.70.4.007
Autor para la correspondencia: Carlos Ramos-Urrea, email: [email protected]
Obesity is known as the major challenge on world’s public health in the 21° century (1), obese teenagers exhibit diseases that were observed only on adults, such as insulin resistance (IR), type 2 diabetes (T2B), hypertension (HTA), metabolic syndrome (MS), sleep apnea, non-alcoholic fatty liver disease (NAFD), among others (2,3). Obesity affects 13% - 20% of the adolescents in occidental countries, and these numbers had presented growth in the last three decades (4), if the growing persists the world will have more obese teenagers than with moderate and severeundernutritionon 2022 (5). Weight excess affects 340 million children and adolescents worldwide, in addition to thedeleterious effects on health, weight excess is associated with a high financial impact on the health system. Obesity is difficult to reverse, and multi-professional strategies are recommended, including dietary, lifestyle changes and the practice differenttypes of physical exercise (6). Only in 2016, an estimated 41 million children under the age of 5 years were overweight or obese (7); in Brazil, recent data showed that approximately 50% of adults and 30% of adolescents present some obesity degree (8), and although the prevalence of malnutrition has decreased considerably in Brazil, it continues to be an important public health problem, especially in some "foci" both in economic abundance as well as in poverty, which are found in large cities. The role of excess weight among children from less privileged social classes is of utmost importance, since these children are not only deprived of a healthy diet, but are also often deprived of culture, education and affection, which causes even greater damage (9).
The weight gain can induce important physical and psychosocial threats toteens' population, because, in this age occurs great changes in body composition, besides that, physical inactivity and poor nutrition can increase the risk of depression and anxiety (2). Physical exercise can improve body composition, metabolic profile and inflammatory state on teenagers with obesity, thus, an important nonpharmacological approach (10), traditionally, two strategies (aerobic and resistance training) had been proposed to obesity damage control, which can improve quality of life, those strategies consist on protocols of resistance and aerobic training (8,11,12).
Both types of training had benefits on multiples valences associated with obesity (11,13–15), however, to the best of our knowledge, few studies on teenagers had compared the two, separated or combinate, and no systematic review had analyzed the effects of both on body composition on obese adolescents. Thus, our aim was to demonstrate, on a systematic review, the effects of the resistance and aerobic training on body composition on adolescents with obesity, as to identify which one is more effective for the analyzed outcomes, to improve the knowledge in this subject, we include studies that combine the two types to compare.
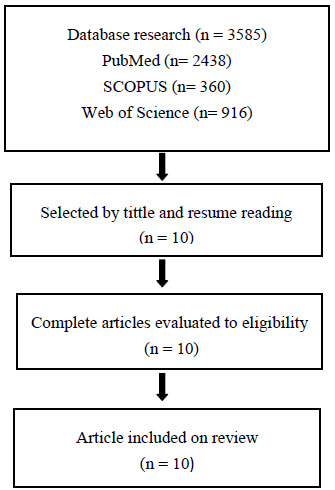
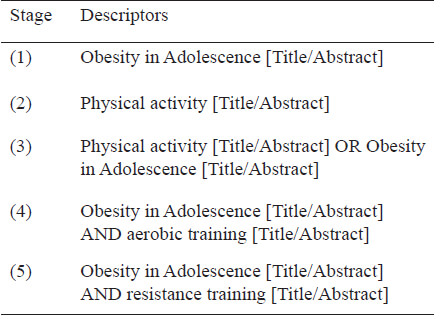
This systematic review is registered on International Prospective Register of Systematic Reviews (PROSPERO) on identification number 146021. We use PICO strategy for eligibility criteria. PEDRo scale was used to bias and quality evaluation. The article selection was on PubMed, SCOPUS e Web of Science databases, using the following descriptors: Obesity, child adolescent, fat mass, body mass index, body mass, intervention, aerobic training, resistance training, physical activity. Posteriorly, the peer review was made by tittle and resumes reading, for this matter, we used Rayyan online platform (https://rayyan.qcri.org/), where also were excluded the duplicates.
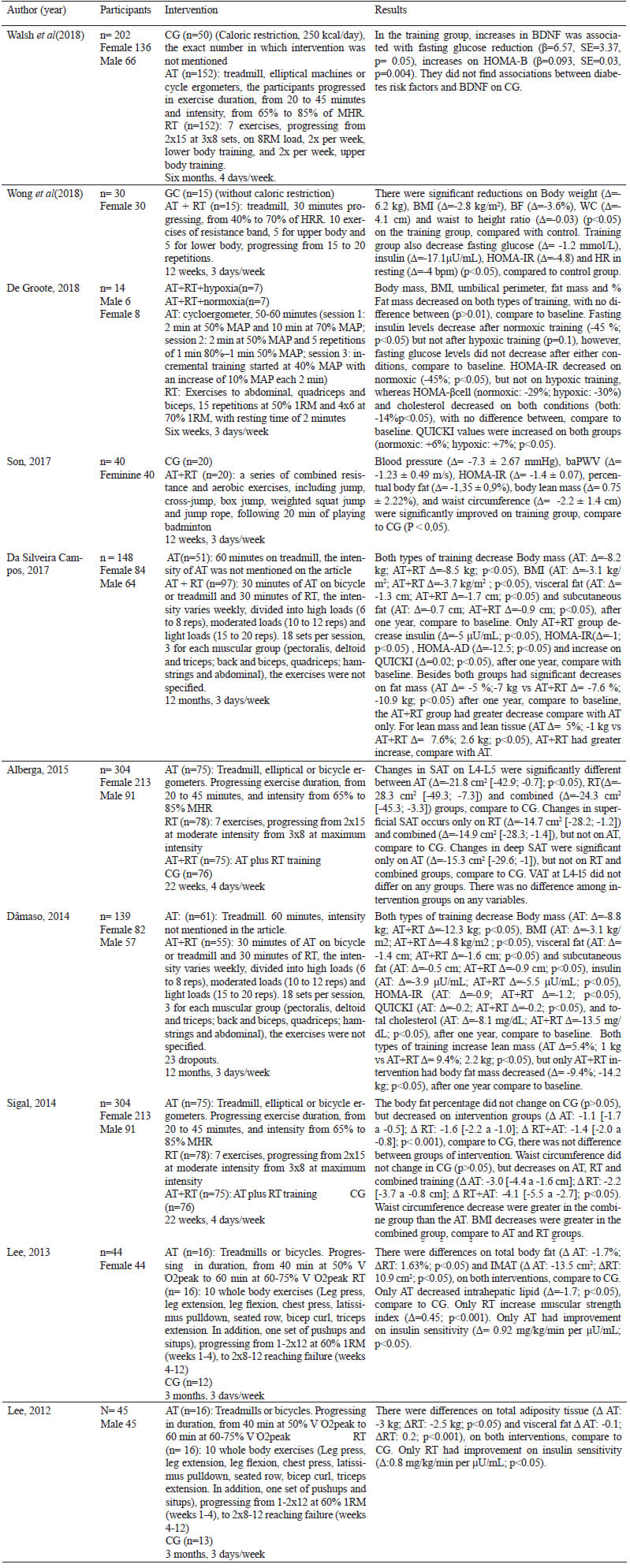
The database research was made in July 2019, with the following inclusion criteria: original articles, disponible on English, Portuguese and Spanish, and that compare the resistance and/or aerobic training in adolescents on the proposed outcomes. As exclusion criteria: systematic reviews and articles without training comparison. Thus, 10 articles were selected to complete reading, all of them were included on the systematic review and meta-analyses.
The resume of the data was exposed on a synoptic chart, in which presents the information about the review outcomes. The comparison between articles were dispose on topics.
Were found 3585 articles on our descriptors analysis, on PubMed (2438), SCOPUS (360) and Web of Science (916), 129 articles were excluded as duplicates. Through the titles and resumes Reading, 10 articles were selected for a complete reading.
To the best of our knowledge this is the first systematic review comparing effects of RT and TA on body composition and obesity outcomes on obese teenagers.
The primary finding was to show that resistance training has significant improvements in muscle mass than aerobic training (SMD= 0.68 vs. 1.37), one of the explanations may be because resistance training can have positive effects on muscle mass, improving hypertrophy, due to a greater stimulation within the cellular activity in the muscle, through a higher volume of exercises, quantitative changes in skeletal muscle mass or fiber diameter and increased muscle strength (16) when compared to aerobic training (improvement in the energy system dependent on oxidative metabolism, qualitative changes in the type of skeletal muscle fiber, metabolic capacity and cardiorespiratory fitness) (17). In addition to our work, we have shown that interventions smaller than 12 weeks by almost 30 minutes composed with aerobic training and resistance training can bring benefits for the improvement of body composition.
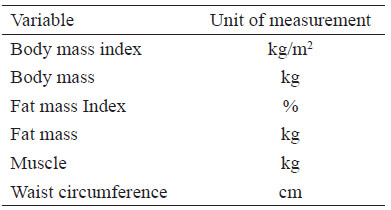
The physical activity guides recommend the combination of AT and RT to optimize the health of the individual, and for other benefits in general (18). Recently the American College of Sport Medicine confirmed that there is evidence to assert that AT and/or RT may promote weight loss (19). Our review study suggests that there are no differences between these two types of training for the decrease of anthropometric parameters such as BMI, fat mass (in percentage and kilograms), PCT, and waist circumference, but itis important to mention that both types of training help decrease these parameters in both sexes and that individuals who underwent resistance training have the same tendency to decrease the percentage of BMI, fat mass and waist circumference as those who underwent aerobic training with a p value < 0.05. Just doing some kind of training can bring benefits within the body composition of an obese individual (20).
According to the World Health Organization (21), for significant weight loss (between 5 and 7 kg per month), it is necessary to practice 225 to 420 min of aerobic exercisesto adolescents, of moderate intensity, per week. In addition, according to the institution mentioned, resistance physical exercise can potentiate the loss of fat mass, when associated with aerobic physical exercises, because it increases or promotes the maintenance of lean mass during the weight loss process, contributing to the increase in resting metabolic rate and daily caloric expenditure; improves functional capacity, facilitating the practice of daily physical activities, and increases lipid oxidation during and especially after physical exercise (22).
Some of the studies cited also used nutritional interventions within the sports interventions in adolescents where (23,24) had a diet regimen based on caloric restriction (55-60% carbohydrates, 15-20% proteins and 20-25% lipids). Another research group (25) also did caloric restriction (Deficit of 250 kcal/day (1.0467kJ), interventions only with caloric restriction seem to lead to greater reductions in BMI when accompanied by some type of training, but changes in BMI may reflect a reduction in BMI dependent on muscle mass rather than fat mass, especially in children involved in physical activity interventions (26). A meta-analysis reported that diet-only interventions resulted in greater BMI reductions than exercise-only interventions among obese children and adolescents. However, without information on changes in lean mass, it is not possible to compare the effectiveness of these interventions, because we do not know if this occurs because the exercise group was gaining lean mass, the group only with diet was losing lean mass, or both (27). Finally, as evidence suggests that exercise-induced changes in energy balance can stimulate compensatory adjustments that alter daily food intake (28), diet control is required during physical activity interventions.
All studies analyzed describe a decrease in waist circumference, which is frequent within interventions that relate abdominal fat to aerobic training and resistance training (23), decreased abdominal fat during adolescence may confer important cardiometabolic protection due to which in an individual each year with abdominal obesity may have a 4% risk for developing diabetes mellitus (23).
Adolescents with obesity have a high adherent to training protocols in both aerobic activities (99.7 ± 0.8%) as in the resistance training group (99.0 ± 2.1%) (23). This observation confirms that the exercise regimen (three times/week or 180 min/week) is feasible and effective for obese adolescents.
Some studies have also been able to measure insulin sensitivity,showing that both aerobic exercise and resistance exercise improve insulin sensitivity, but to present differences between them when compared to the control group (25). Other researchers (23) have achieved that aerobic training maintained insulin sensitivity, and that it is demonstrate that resistance exercise sessions 2 to 3 times a week can increase insulin sensitivity by a 27% (29).
None of the study’s findings report on the prevention of weight recovery, in none there was monitoring of weight after studies, and it is that some research shows that the maintenance of the new weight acquired is as arduous a task as the weight loss process itself (22), more studies that elude the volume, intensity and the best types of physical exercise are essential. According to other measured parameters, we have that both AT and RT can improve BDNF being an effective strategy for brain health (30), the TA shows to be more effective for the improvement of the HOMA-IR index (8)when compared to TA, TR, and combined training we believe that the three improve abdominal adiposity in the population studied (28) although we do not compare different types of training when the combined exercises were studied in isolation, we have that they can show improvement in arterial stiffness, nitric oxide values and inflammatory markers, these findings were only evaluated in obese girls (31). When this type of exercise (Combined) and performed in hypoxia shows that it can be an interesting strategy against IR and development of DM2 in both sexes (32). Combined exercise proves to be a useful therapeutic treatment for high BP, IR, central and visceral adiposity, hepatic markers at ApoB / ApoA-1 ratio (12,15,31,33). Aerobic and resistance exercises performed with protocols of 3 to 4 weekly trainings, with sessions of 15 to 60 minutes in interventions from 4 to 12 weeks with caloric restriction resulted in reductions in the parameters analyzed, the two types of training allow greater use of fat stocks as an energetic substrate and preserves lean mass (34).
There is already consensus in the literature that strategies involving physical exercise, food reeducation and behavioral changes jointly are more effective in the treatment of obesity than such practices performed in isolation(35,36), although not included in any guide, it is necessary that the members of the obesity treatment teams are well trained and have specific competencies, especially during the practical approach of patients (37).
It is relevant to mention the sex differences, which six of ten studies analyzed both sexes, but only one compared them, reveling that gender did not moderate the effects of exercise on BDNF or diabetes risk factor, and did not function as confounder by the BDNF, fasting glucose and HOMA-B changes in the exercise group, as well as, there was no difference between sex on adherence in exercise programs (30). Howsoever, two of the studies selected (Table 3), had both sex in the sample, but they did not analyzed difference among them (31,38).
It would be important to develop others study of this type with combined exercise, since the most frequent recommendations within physical exercise for the treatment of obesity have to be composed of strength training, with a large number of repetitions in conjunction with moderate intensity aerobic training, showing to be more efficient in improving the body composition of adolescents with obesity (39,40). The main limitation of this work was the small number of articles obtained, demonstrating once again the need to study the effect of different types of training in adolescents with obesity.
It is important that the adolescent with obesity who craves weight loss, maintenance of new body weight and incorporation of a healthy life find and practice pleasurable physical activities, which facilitate adherence to a more active life.
The treatment of obesity should address lifestyle changes that include:
Food reeducation, increased practice of physical exercise, behavioral changes, pharmacological intervention (when necessary) and environmental changes.
Adolescents who want to maximize the effect of exercise on anthropometric variables should ideally perform aerobic and endurance exercises, but significant benefit can be achieved through any type of exercise, and if it were to have a significant differentiation within muscle mass the resistance exercise may be ideal to achieve this goal.
It would be of great importance to evaluate variables related to the pubertal stretch stage (Tanner's stage) for this target population so that from there we can make more accurate decisions regarding exercise protocols and thus optimize transdisciplinary work, this due to the endocrine-metabolic influence, which has a fundamental role, which will set the pattern of development according to the levels of maturation, early, average and late. In none of the studies analyzed has it been documented about the influence of obesity within the development period, considering the distribution of fat and lean mass.
We are grateful to Prof. Thatiane Ostolin for helping us and for her generous support and all the education help.
This research was not funded by any agency.
The authors declare that there are no conflicts of interest in this paper.
The authors’ contributions are as follows: T.G.C, L.R. and C.R.U. designed the study. C.R.U. and T.G.C. performed all data collection. L.R. completed all tables, and interpreted the data, C.R.U. and T.G.C. wrote the paper. T.G.C. contributed to revision of the paper. T.G.C. and C.R.U. contributed to the writing and discussion of the paper. All authors were responsible for the critical revisions of the paper and approved the final version.
Recibido: 05/10/2020
Aceptado: 10/03/2021