Introduction
Insulin resistance (IR) is characterized by a decrease in the capacity of insulin to perform its normal physiological functions. It usually appears before type 2 diabetes mellitus or metabolic syndrome and is associated with overweight and obesity (1). Other factors also associated with it are age, gestation, and polycystic ovary – where IR also plays an important role (2).
At first, IR creates compensatory mechanisms so that, for a time, increased insulin secretion manages to keep blood glucose levels under control (3). This period, which we could call pre-diabetic, is difficult to detect clinically, because blood glucose levels are normal; however, this situation progressively worsens when pancreatic failure appears, that is, when the beta cells of the pancreas are not only incapable of maintaining insulin hypersecretion, but also begin to deteriorate, thereby decreasing insulin secretion. In this situation most cases of type 2 diabetes mellitus and metabolic syndrome are diagnosed. It is also known that genetic (4) and oxidative stress (5) mechanisms are involved in the genesis of IR.
Insulin not only regulates glucose homeostasis, but also plays an important role in lipid and protein metabolism, which in turn can be altered in states of insulin resistance (6).
The aim of this study was to determine how healthy habits (physical activity, Mediterranean diet, and tobacco consumption) and sociodemographic variables (age, sex, and social class) affect cardiometabolic profile.
Material and methods
A retrospective, cross-sectional study was performed in 1584 Spanish workers during the period from January 2017 to December 2017. Of these, 127 were excluded (69 for not agreeing to participate and 58 for being under 18 years of age) remainding 1457 workers who were the ones finally included in the study; 718 of these were women (mean age 43.30 years) and 739 men (mean age 46.02 years). The workers were selected from among those who attended periodic occupational medical check-ups.
Inclusion criteria
- Aged between 18 and 67 years.
- Being an active worker.
- Belonging to one of the companies collaborating in the study.
- Accepting to participate in the study.
Anthropometric measurements of height and weight, both clinical and analytical, were performed by the health personnel of the different occupational health units participating in the study, after standardizing the measurement techniques. These measurements are performed according to ISAK criteria (7).
To measure weight, expressed in kilograms, and height, which is expressed in m, a scale with a measuring rod was used: SECA brand 700 with a SECA 220 telescopic measuring rod attached.
Abdominal waist circumference was measured with a SECA model measuring tape with the person in a standing position, feet together, trunk erect, and abdomen relaxed. The tape was placed parallel to the floor at the level of the last floating rib. Hip circumference is measured at the level of the femoral trochanters coinciding with the point where the buttocks reach the greatest development. Waist to height ratio and waist to hip ratio indices were obtained by dividing the waist circumference by height and hip circumference, respectively. The cut-off point for the former was 0.50 and for the latter 0.85 for women and 0.95 for men (8).
Blood pressure was measured lying down with a calibrated OMRON M3 automatic sphygmomanometer after 10 minutes of rest. Three measurements were taken at one-minute intervals and the mean of the three was used. Blood tests were obtained by peripheral venipuncture after a 12-hour fast. Samples were sent to reference laboratories and processed within 48-72 hours. Automated enzymatic methods were used for blood glucose, total cholesterol, and triglycerides. Values are expressed in mg/dl. HDL was determined by precipitation with dextran sulfate Cl2Mg, and values were expressed in mg/dl. LDL was calculated using the Friedewald formula (provided that triglycerides were below 400 mg/dl). Values are expressed in mg/dl.
Friedewald formula: LDL= total cholesterol – HDL – triglycerides/5
Glycemia figures were classified based on the recommendations of the American Diabetes Association (9); patients with a previous diagnosis, those who after obtaining a glycemia figure higher than 125 mg/dl presented glycosylated hemoglobin ≥ 6.5%, and those on hypoglycemic treatment were qualified as diabetic.
Body mass index (BMI) is calculated by dividing weight by height in meters squared (BMI= Weight (kg)/Height² (m)). The cut-off point for obesity according to WHO criteria is 30.
Lipid accumulation product (LAP) (10) is calculated:
- In men: (waist circumference (cm) – 65) x (triglyceride concentration (mMol)).
- In women: (waist circumference (cm) – 58) x (triglyceride concentration (mMol)).
The cut-off point for it to be considered high is 30.40 in women and 56.70 in men (11).
Cardiometabolic index (12) is obtained by multiplying the waist-to-height ratio by the triglyceride/HDL-c atherogenic index. The cut-off point for considering it high is 0.80 for women and 1.75 for men.
Waist triglyceride index (13) is calculated by multiplying the waist circumference in cm by triglycerides in mmol. The cut-off point is 190.40. triglyceride glucose index – BMI, triglyceride glucose index – waist circumference
Ty G index (14) = LN (TG [mg/dL] × blood glucose [mg/dL]/2). With a cut-off point of 8.72 in men and 8.92 in women (15).
Other indices are derived from it (16).
Ty G index-BMI = Ty G index x BMI
Ty G index- waist circumference = Ty G index x waist circumference
Ty G index-waist to height ratio= Ty G index x waist/height
Ty G index-waist/hip
Tobacco consumption was considered as a dichotomous variable and could have the value of yes/no. A smoker was a person who had regularly consumed at least 1 cigarette/day (or the equivalent in other types of consumption) in the previous month or had quit smoking less than a year before. A person who had not smoked for more than 12 months or had never smoked was considered a non-smoker.
Social class was obtained from the 2011 National Classification of Occupations (CNO-11), based on the proposal made by the social determinants group of the Spanish Society of Epidemiology (17). We opted for classification in 3 categories: Class I, Directors/managers, university professionals, athletes and artists. Class II, Intermediate occupations and self-employed workers without employees. Class III, Unskilled workers.
Diet was assessed by means of the questionnaire on adherence to the Mediterranean diet (18) based on the Predimed test, which consists of 14 questions that are scored with 0 or 1 point each. Values below 9 are considered low adherence and values of 9 or higher are considered good adherence.
The International Physical Activity. Questionnaire (19) (IPAQ) consists in questions about the frequency, duration and intensity of activity (moderate and intense) performed in the last seven days, as well as walking and sitting time in a working day. The short 7-item version is used in this study.
TEST VALUE:
- Walking: 3'3 METx minutes of walking x days per week.
- Moderate Physical Activity: 4 MET*x minutes x days per week
- Vigorous Physical Activity: 8 MET*x minutes x days per week.
The three values obtained are then added together
CLASSIFICATION CRITERIA:
Moderate Physical Activity:
- 3 or more days of moderate physical activity and/or walking at least 30 minutes per day.
- 5 or more days of any combination of walking, moderate or vigorous physical activity achieving at least a total of 600 METs.
Vigorous Physical Activity:
- Vigorous Physical Activity at least 3 days per week achieving a total of at least 1500 METs.
- 7 days of any combination of walking, moderate physical activity and/or vigorous physical activity, achieving a total of at least 3000 METs.
MET is the Unit of Measurement of the test
Statistical analysis
A descriptive analysis of the categorical variables was performed, by calculating the frequency and distribution of responses for each one. For quantitative variables, the mean and standard deviation were calculated, while for qualitative variables, the percentage was calculated. The bivariate association analysis was performed using the Chi squared test (with correction of Fisher's exact statistic when conditions required it) and Student's t test for independent samples. For the multivariate analysis, binary logistic regression was used with the Wald method, with calculation of the Odds ratio and the Hosmer-Lemeshow goodness-of-fit test. Statistical analysis was performed with the SPSS 27.0 program, with an accepted statistical significance level of 0.05.
Ethical considerations and aspects
The study was approved by the Clinical Research Ethics Committee of the Balearic Islands Health Area no. IB 4383/20. All procedures were performed in accordance with the ethical standards of the institutional research committee and with the 2013 Declaration of Helsinki. All patients signed written informed consent documents before participating in the study.
Results
Values of the anthropometric, clinical, analytical, sociodemographic, and healthy habit variables, with the exception of cholesterol, were worse among the men in our study population. The complete data are presented in Table 1.
Table 1. Characteristics of the population
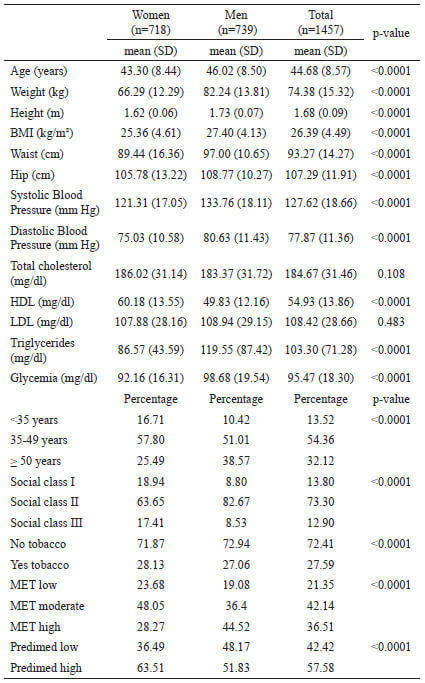
BMI Body mass index. HDL High Desity Lipoprotein. LDL. Low Density Lipoprotein. MET Unit of Measurement of the IPAQ questionnaire. MET low under 600 METS, MET moderate between 600-2999 MET, MET high at least 3000 MET Predimed low ≤ 8 points Predimed high ≥ 9 points.
Most of the scales studied showed an improvement in mean values as the level of physical activity increased; this situation was observed in both sexes. The complete data are presented in Table 2.
Table 2. Mean values in the different scales according to physical activity by gender
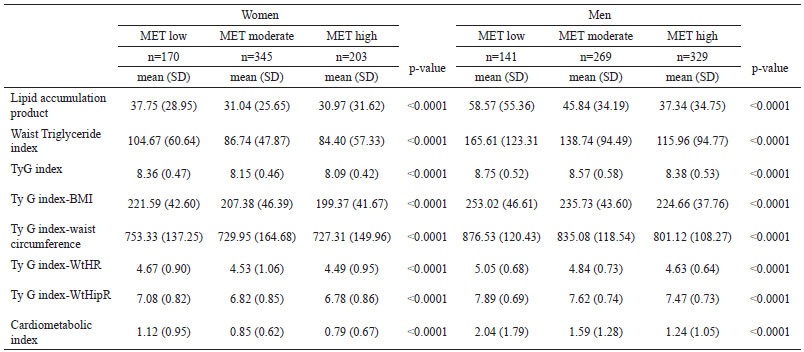
Ty G Triglyceride Glucose index WtHR Waist to Height Ratio. WtHipR Waist to Hip Ratio. BMI Body mass index. MET Unit of Measurement of the IPAQ questionnaire. MET low under 600 METS, MET moderate between 600-2999 MET, MET high at least 3000 MET
Something similar was observed with adherence to the Mediterranean diet, such that people, both men and women, with high adherence presented better values in the scales analyzed. All the data are shown in Table 3.
Table 3. Mean values in the different scales according to healthy food by gender
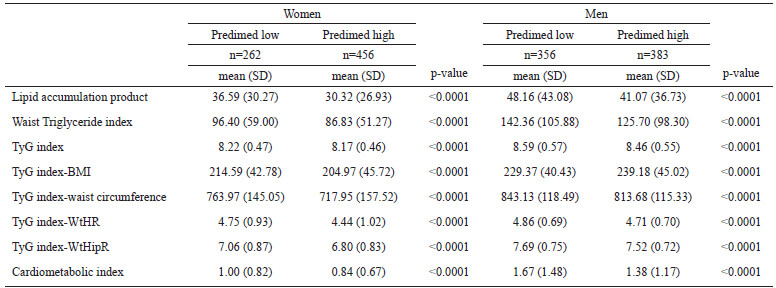
Ty G Triglyceride Glucose index WtHR Waist to Height Ratio. WtHipR Waist to Hip Ratio. BMI Body mass index Predimed low ≤ 8 points Predimed high ≥ 9 points
As occurred with the mean values, the prevalence of altered values in these scales decreased in parallel with an increase in the level of physical activity, which could be seen in both women and men (see Table 4).
Table 4. Prevalence of altered values in the different scales according to physical activity by gender
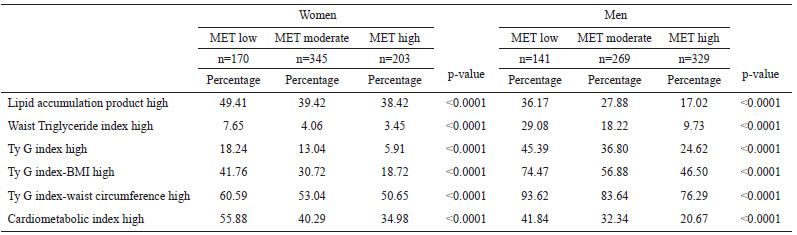
Ty G Triglyceride Glucose index. BMI Body mass index. MET Unit of Measurement of the IPAQ questionnaire. MET low under 600 METS, MET moderate between 600-2999 MET, MET high at least 3000 MET
Adherence to the Mediterranean diet had a similar effect on the prevalence of the values studied in these scales, with better results in people with a high adherence, as shown in Table 5.
Table 5. Prevalence of altered values in the different scales according to healthy food by gender
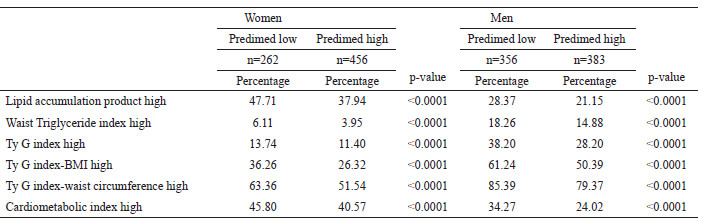
Ty G Triglyceride Glucose index. BMI Body mass index Predimed low ≤ 8 points Predimed high ≥ 9 points
Age over 50 years, male sex, smoking, low physical activity, low adherence to the Mediterranean diet, and social classes II and III were established as covariates in the multivariate analysis, with sex and physical activity as the only variables that displayed an influence in all the scales analyzed.
Of these, the one showing the greatest influence was sex, with odds ratios ranging from 0.36 (95% CI 0.28-0.46) for LAP to 4.34 (95% CI 2.90-6.50) for high Waist Triglyceride index. On the other hand, tobacco only showed a relationship with Ty G index-BMI. All the results are presented in Table 6.
Table 6. Logistic regression analysis
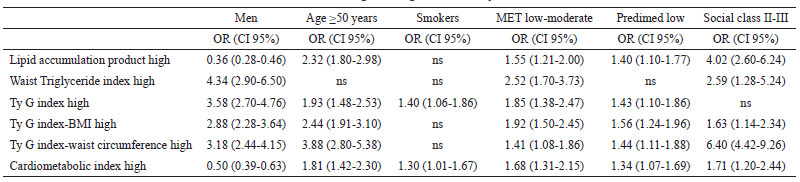
Ty G Triglyceride Glucose index. BMI Body mass index. Ns. Non significance. MET Unit of Measurement of the IPAQ questionnaire Predimed low ≤ 8 points . MET low under 600 METS, MET moderate between 600-2999 MET.
Discussion
In our study, both the mean values and the prevalence of altered values in the different scales that assess insulin resistance decreased as the level of physical activity assessed with the IPAQ questionnaire and adherence to the Mediterranean diet increased.
In the studies consulted, following our review of the literature, few address the influence of healthy habits and sociodemographic variables on the values of the scales that determine insulin resistance as we do in this study.
When it comes to assessing the effect of physical activity on insulin resistance, we find different results, although most of them consider that it has a beneficial effect. Thus, a cross-sectional study performed in 90 Brazilian patients in 2015 (20) that evaluated lipid accumulation product values and their relationship with different variables, including physical activity determined with the IPAQ questionnaire, showed that this parameter increased as the level of exercise decreased in a similar way to what we found in our work, although the mean age of the population in our study is younger. This same beneficial effect has been observed in other research such as that of Sampath Kumar (21) who in a meta-analysis of 2019 where data from 846 people included in structured physical exercise programs were analyzed, concluded that the mean insulin resistance values decreased in the group that performed exercise compared to those who did not. In the same sense we find the study by Whillier (22), although in this case it is not clear whether the positive effect on insulin resistance is due to the physical exercise itself or whether it is due to the loss of weight or visceral fat.
Amanat et al (23) conducted a study in 66 overweight women with metabolic syndrome in which they assessed the effect of different types of physical exercise for 12 weeks (aerobic, resistance and combined) and observed that in all three cases there was a decrease in insulin resistance when compared to the control group that did not do physical exercise. Dalmazzo et al (24) compared the impact of a high intensity intervallic training program versus a muscular resistance training program on insulin resistance in 28 Chilean adults, observing a lower insulin resistance in both cases (25). Other studies found this same beneficial effect of high-intensity interval training on insulin resistance (26-28), as well as with muscular endurance programs (29-30).
However, we also found research that did not find any improvement in insulin resistance values in people who performed physical exercise. A study by Fedewa et al. (31) carried out in 44 overweight people who performed moderate or vigorous physical exercise found improvements in HDL and LDL cholesterol values but not in insulin resistance values.
If we focus on the effects of the Mediterranean diet on insulin resistance, we find two studies that corroborate the beneficial effect of this type of diet as we have found. Mirabelli (32) observed that in obese people the Mediterranean diet improved insulin resistance values when compared with other types of diet. On the other hand, Papadaki (33) in a meta-analysis involving almost 37,000 people found beneficial effects of the Mediterranean diet on the different components of the metabolic syndrome, including insulin resistance.
Other studies have assessed the combined effect of physical activity and the Mediterranean diet on insulin resistance values. Sánchez-Escudero et al studied 60 young people aged 7 to 16 years (34) whose adherence to the Mediterranean diet and amount of physical activity were assessed using the International Sedentary Assessment Tool (ISAT) and Actigraph wGT3X+ accelerometers, revealing lower values of insulin resistance -determined with the Triglyceride Glucose index- in those who performed moderate-vigorous physical activity. These data are similar to those of our study, although here too the age of the population is different. Malakou (35) carried out a systematic review with meta-analysis in more than 1600 people and also observed this beneficial effect on insulin resistance.
A fundamental limitation of the study is the fact that, being a working population, it does not include unemployed, retired, under 18 years of age or over 67 years of age, so that the results cannot be extrapolated to the general population as they are not representative of it.
Among the strengths of this study are the large sample size, the high number of insulin resistance scales analyzed, and the fact that the assessment of physical activity and adherence to the Mediterranean diet was performed with validated questionnaires (IPAQ and Predimed).
Conclusions
The cardiometabolic profile, including insulin resistance, of persons with high levels of physical activity determined with the IPAQ questionnaire and of persons with high adherence to the Mediterranean diet is better than that of sedentary persons with low adherence to the Mediterranean diet.
This beneficial effect is observed separately with each of these healthy habits and a synergistic effect is also observed when both are presented together.
References
- Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the United States. JAMA. 2001;286(10):1195-1200.
- Facchini FS, Hua N, Abbasi F, Reaven GM. Insulin resistance as a predictor of age-related diseases. J Clin Endocrinol Metab. 2001;86(8):3574-3578.
- Reaven GM. The insulin resistance syndrome: definition and dietary approaches to treatment. Annu Rev Nutr. 2005; 25:391-406.
- Voight BF, Scott LJ, Steinthorsdottir V, Morris AP, Dina C, Welch RP, et al. Twelve type 2 diabetes susceptibility loci identified through large-scale association analysis. Nat Genet. 2010;42(7):579-589.
- Lowell BB, Shulman GI. Mitochondrial dysfunction and type 2 diabetes. Science. 2005;307(5708):384-387.
- Schenk S, Saberi M, Olefsky JM. Insulin sensitivity: modulation by nutrients and inflammation. J Clin Invest. 2008;118(9):2992-3002.
- Vidal Pérez D, Martínez-Sanz JM, Ferriz-Valero A, Gómez-Vicente V, Ausó E. Relationship of Limb Lengths and Body Composition to Lifting in Weightlifting. Int J Environ Res Public Health. 2021;18(2):756.
- Luengo Pérez LM, Juan Manuel Urbano Gálvez JM, Pérez Miranda M. Validación de índices antropométricos alternativos como marcadores del riesgo cardiovascular. Endocrinol Nutr. 2009;56(9):439-46
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care. 2020;43(Suppl 1): S14-S31
- Chiang JK, Koo M. Lipid accumulation product: a simple and accurate index for predicting metabolic syndrome in Taiwanese people aged 50 and over. BMC Cardiovasc Disord. 2012; 12:78
- Ahn N, Baumeister SE, Amann U, Rathmann W, Peters A, Cornelia C, et al. Visceral adiposity index (VAI), lipid accumulation product (LAP), and product of triglycerides and glucose (TyG) to discriminate prediabetes and diabetes. Scientific Reports 2019; 9:9693
- Wakabayashi I, Daimon T. The "cardiometabolic index" as a new marker determined by adiposity and blood lipids for discrimination of diabetes mellitus. Clin Chim Acta. 2015;438:274-278.
- Yang RF, Liu XY, Lin Z, Zhang G. Correlation study on waist circumference-triglyceride (WT) index and coronary artery scores in patients with coronary heart disease. Eur Rev Med Pharmacol Sci. 2015;19(1):113-118
- Unger G, Benozzi SF, Peruzza F, Pennacchiotti GL. Triglycerides and glucose index: A useful indicator of insulin resistance. Endocrinol Nutr. 2014;61(10):533-40
- Ramírez-Vélez R, Pérez-Sousa MA, González-Ruíz K, Cano-Gutiérrez CA, Schmidt-RioValle J, Correa-Rodríguez M, et al. Obesity- and Lipid-Related Parameters in the Identification of Older Adults with a High Risk of Prediabetes According to the American Diabetes Association: An Analysis of the 2015 Health, Well-Being, and Aging Study. Nutrients. 2019; 11(11):2654.
- Zheng S, Shi S, Ren X, Han T, Li Y, Chen Y, et al. Triglyceride glucose-waist circumference, a novel and effective predictor of diabetes in first-degree relatives of type 2 diabetes patients: cross-sectional and prospective cohort study. J Transl Med 2016; 14(1):260.
- Domingo-Salvany A, Bacigalupe A, Carrasco JM, Espelt A, Ferrando J, Borrell C. Propuesta de clase social neoweberiana y neomarxista a partir de la Clasificación Nacional de Ocupaciones 2011. Gac Sanit 2013;27(3):263-272
- Miró Ò, Martín-Sánchez FJ, Jacob J, Andueza JA, Herrero P, Llorens P. Valoración del grado de adherencia a la dieta mediterránea en pacientes con insuficiencia cardiaca: Estudio DIME-EAHFE. An Sist Sanit Navar 2016;39(2): 261-8
- Seron P, Muñoz S, Lanas F. Nivel de actividad física medida a través del cuestionario internacional de actividad física en población chilena. Rev Med Chile. 2010;138(10):1232-1239.
- Vieira BA, Sauer P, Mercadent A, Haas-Piovesant C. Association between LAP Index (lipid accumulation product) and metabolic profile in hospitalized patients. Nutr Hosp. 2015;31(6):2771-2774
- Sampath Kumar A, Maiya AG, Shastry BA, Vaishali K, Ravishankar N, Hazari A et al. Exercise and insulin resistance in type 2 diabetes mellitus: A systematic review and meta-analysis. Ann Phys Rehabil Med. 2019;62(2):98-103.
- Whillier S. Exercise and Insulin Resistance. Adv Exp Med Biol. 2020; 1228:137-150.
- Amanat S, Sinaei E, Panji M, MohammadporHodki R, Bagheri-Hosseinabadi Z, Asadimehr H, et al. A Randomized Controlled Trial on the Effects of 12 Weeks of Aerobic, Resistance, and Combined Exercises Training on the Serum Levels of Nesfatin-1, Irisin-1 and HOMA-IR. Front Physiol. 2020;11:562895.
- Dalmazzo V, Ponce A, Delgado-Floody P, Carrasco-Alarcón V, Martínez-Salazar C. Efectos del ejercicio físico intervalado en la mejora del control glicémico de adultos obesos con insulinorresistencia. Nutr. Hosp 2019; 36(3): 578-582.
- Madsen SM, Thorup AC, Overgaard K, Jeppesen PB. High intensity interval training improves glycaemic control and pancreatic beta cell function of type 2 diabetes patients. PLoS One 2015;10(8): e0133286.
- Robinson MM, Dasari S, Konopka AR, Johnson ML, Manjunatha S, Esponda RR, et al. Enhanced protein translation underlies improved metabolic and physical adaptations to different exercise training modes in young and old humans. Cell Metab 2017;25(3):581-592.
- Burgomaster KA, Howarth KR, Phillips SM, Rakobowchuk M, Macdonald MJ, McGee SL, et al. Similar metabolic adaptations during exercise after low volume sprint interval and traditional endurance training in humans. J Physiol 2008;586(1):151-160.
- Zapata-Lamana R, Cigarroa I, Díaz E, Saavedra C. Reducción del riesgo cardiovascular en mujeres adultas mediante ejercicio físico de sobrecarga. Rev Med Chile 2015; 143:289-296.
- Delgado-Floody P, Caamaño-Navarrete F, Jerez-Mayorga D, Martínez-Salazar C, García-Pinillos F, Latorre-Román P. Adaptaciones al ejercicio físico en el perfil lipídico y la salud cardiovascular de obesos mórbidos. Gac Med Mex 2017;153(7):781-786.
- Pesta DH, Goncalves RL, Madiraju AK, Strasser B, Sparks LM. Resistance training to improve type 2 diabetes: working toward a prescription for the future. Nutr Metab 2017;14 (1):24.
- Fedewa MV, Hathaway ED, Higgins S, Forehand RL, Schmidt MD, Evans EM. Moderate, but not vigorous, intensity exercise training reduces C-reactive protein. Acta Cardiol. 2018;73(3):283-290.
- Mirabelli M, Chiefari E, Arcidiacono B, Corigliano DM, Brunetti FS, Maggisano V, et al. Mediterranean Diet Nutrients to Turn the Tide against Insulin Resistance and Related Diseases. Nutrients. 2020;12(4):1066.
- Papadaki A, Nolen-Doerr E, Mantzoros CS. The Effect of the Mediterranean Diet on Metabolic Health: A Systematic Review and Meta-Analysis of Controlled Trials in Adults. Nutrients. 2020;12 (11): 3342.
- Sánchez-Escudero V, García Lacalle C, González Vergaz A, Remedios Mateo L, Marqués Cabrero A. The triglyceride/glucose index as an insulin resistance marker in the pediatric population and its relation to eating habits and physical activity. Endocrinol Diabetes Nutr. 2021;68(5):296-303.
- Malakou E, Linardakis M, Armstrong MEG, Zannidi D, Foster C, Johnson L, et al. The Combined Effect of Promoting the Mediterranean Diet and Physical Activity on Metabolic Risk Factors in Adults: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients. 2018;10(11):1577.