Introduction
While assessment of an individual’s health status is challenging, self-perceived health (SPH) is associated with objective health measures, such as laboratory, physical, and cognitive tests (1). Ailing SPH is associated with increased mortality (2-4) and increased prevalence of one or more morbidities, such as diabetes (5,6), cardiovascular diseases (7,8), obesity (9), and other non-communicable health problems (6,10,11). SPH has been considered a good predictor of the general health condition of individuals (1) and is an epidemiological measure that has shown good reproducibility when applied to different populations (12, 13).
Current research on SPH has aimed to relate SPH with lifestyle variables (14-19) and has tested the association with behavioral variables, such as physical inactivity (11,14), alcohol abuse (14,20), eating behaviors (14-19), and tobacco use (14,21).
Regarding studies on eating behaviors, most of them use one or a few food indicators. The most common behavior evaluated is the consumption of fruits and vegetables (14,20-24). Among the eating behaviors considered are the consumption of dietary fats (22,25,26), consumption of eggs and legumes (15,20), and breakfast (18,27). Studies on the relationship between eating behaviors and SPH in adolescents (18,19,27), university students (17), and older adults (15,20,28) are frequent while scarce in young and middle-aged adults (22,26). Few studies cover different age groups (11,23) and very rarely analyze the relationship between SPH and eating behaviors (23). Studies that performed some stratification by age found significant variations between associations (11, 23).
A higher number of associations was found in adults (20-64 years) (11) in a study carried out with Brazilians relating SPH to health behaviors and morbidities. Another study carried out in Greece observed a more significant number of associations between the studied eating behaviors and SPH in younger individuals (15-29 years) than the other age groups (30 to 49 years and over 50 years of age) (23).
Given this context, this study aimed to analyze the association between seven eating behaviors and SPH in young, middle-aged, and older Brazilian adults.
Materials and methods
It is a cross-sectional study from the database of the 2017 Surveillance System for Risk and Protection Factors for Chronic Diseases (VIGITEL). VIGITEL has been conducted annually since 2006 and is a telephone survey in the 26 capitals of the Brazilian states and the Federal District. The sample is probabilistic. The sample is probabilistic. Residents aged 18 years or more, selected from the local telephone listings, were interviewed. For each capital, samples generally consisted of about 2000 individuals. The 2017 survey interviewed 52631 individuals (29).
The dependent variable of this study was positive SPH, obtained through the question “Would you rate your health status as?” with the following response options: Excellent; Good; Fair; Poor; Very Poor. The responses were dichotomized into positive and negative SPH. Those who answered “excellent” and “good” were considered with positive SPH and those who answered “fair”, “poor”, and “very poor” with negative SPH.
The independent variables were seven eating behaviors: exchanging lunch for snacks (never/rarely; 1-7 days a week); exchanging dinner for snacks (never/rarely; 1-7 days a week); bean consumption (≥5 days a week; <5 days a week); consumption of ultra-processed food in the previous day (yes; no); fruit consumption (≥5 days a week; <5 days a week); vegetable consumption (≥5 days a week; <5 days a week); consumption of processed juices and soft drinks (never/rarely; 1-7 days a week). These same eating patterns were considered in the construction of a score, where the number of healthy behaviors for each subject was evaluated so that this score can vary between 0 and 7, this score has not been previously validated by another study. These eating behaviors were available for analysis in the VIGITEL database initially with the categories 1 to 2 days a week; 3 to 4 days a week; 5 to 6 days a week; every day; almost never; never. The categorization of the variables was arbitrary, except for the consumption of fruits and vegetables, which is more commonly observed in the literature with the dichotomization used (14, 29).
In the question regarding the consumption of ultra-processed food the previous day, intake of stuffed biscuits, snacks, sausages, and instant noodles was considered as consumption of ultra-processed food. Other foods fall into this classification, but only the consumption of these four foods was considered due to limitations of the studied database.
Other variables were analyzed to describe the sample and perform the control for possible confounding factors: gender (female/male), age (in years), skin color (white/black/brown/yellow/indigenous), marital status (single/married or common-law marriage/widowed/separated), schooling (in full years), reported morbidity (diabetes, hypertension, obesity), and health behaviors (leisure physical activity, alcohol abuse, and tobacco use).
All tested associations were stratified by gender and three different age groups: young, middle-aged, and older adults, where young adults range from 18 to 39 years, middle-aged adults from 40 to 59 years, and older adults 60 years and over. The choice of age groups was arbitrary, as the definition of middle age is still scarce, while the senile phase is usually adopted after 60 years old (30).
The Wald method calculated the prevalence ratio (PR), considering the 95% confidence interval (95% CI). The adjusted prevalence ratio (PRadj) was calculated using the Poisson regression with robust adjustment for variance. To this end, a regression model was built and included the sociodemographic, referred morbidity, and behavioral variables. All analyses were performed using the SPSS vs. 19.0. The procedures related to VIGITEL were approved by the National Human Research Ethics Committee of the Brazilian Ministry of Health (29).
Results
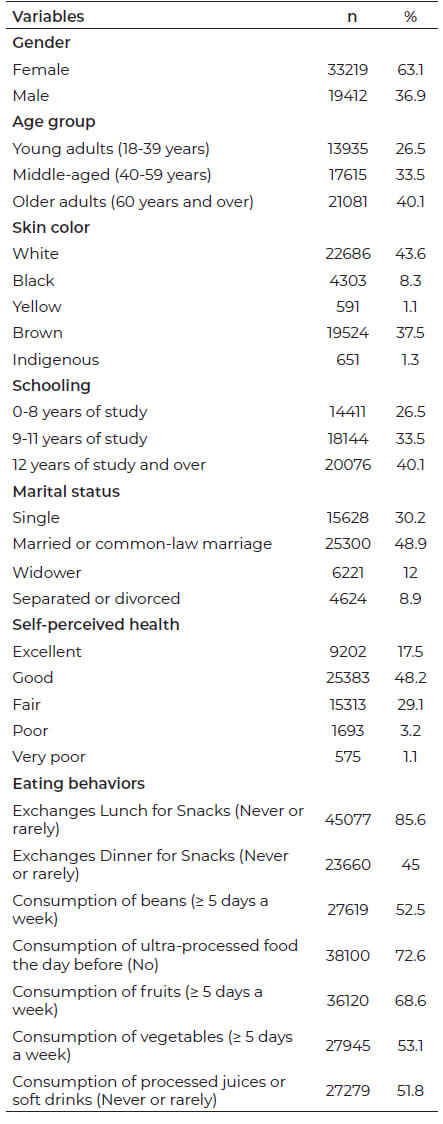
In 2017, 465 of 52166 VIGITEL respondents did not answer the specific question about SPH and were excluded from this study. Most of the respondents were female (63.1 %), 47.5 % were self-referred as white, 48.0 % lived with their partner, and 40.1 % were 60 years of age or older. Concerning SPH, 17.6 % referred to their health as “excellent”, 48.7 % as “good”, 29.4 % as “fair”, 3.2 % as “poor”, and 1.1 % as “very poor” (Table 1).
Table 1: Distribution of the sample, according to social and demographic variables. VIGITEL, Brazil, 2017. (n = 52631).
SPH was associated with all seven eating behaviors studied in young adult women. In middle-aged women, only the variables related to the consumption of fruits and vegetables were associated with SPH. For older adults were equally concerning these same variables (fruits and vegetables) along with exchanging lunch and dinner for snacks. Of these associations, the prevalence of positive SPH was higher among those with healthy eating behaviors, except for exchanging dinner for snacks in older adults, where older women who reported never or rarely exchanging dinner for snacks had a lower prevalence of positive SPH than those who referred to carrying out this exchange 1-7 days a week (Table 2).
Table 2: Association between food consumption and positive self-perceived health in women living in Brazilian capitals. VIGITEL, Brazil, 2017. (n = 33219).
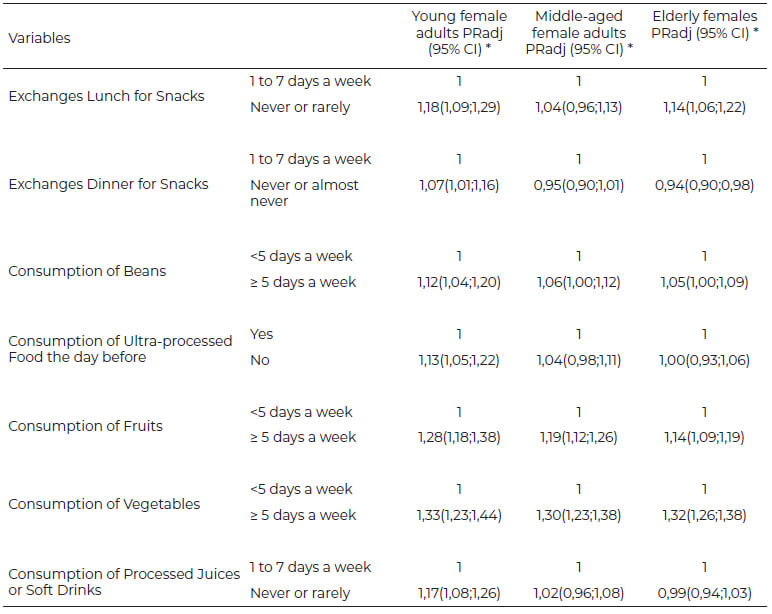
95% CI: 95% Confidence Interval.
* Adjustment of variables for gender, age, skin color, marital status, schooling, diabetes, hypertension, obesity, leisure-time physical activity, alcohol abuse, and tobacco use.
Concerning men, the results were similar to those observed in women. All eating behaviors were associated with SPH in young adults, while middle-aged men showed an association with the consumption of fruits, vegetables, and beans, and older adults, only with fruits and vegetables. In all of these associations, the prevalence of positive SPH was higher among those with healthy eating behaviors (Table 3).
Table 3: Association between food consumption and positive self-perceived health in men living in Brazilian capitals. VIGITEL, Brazil, 2017. (n = 19412).
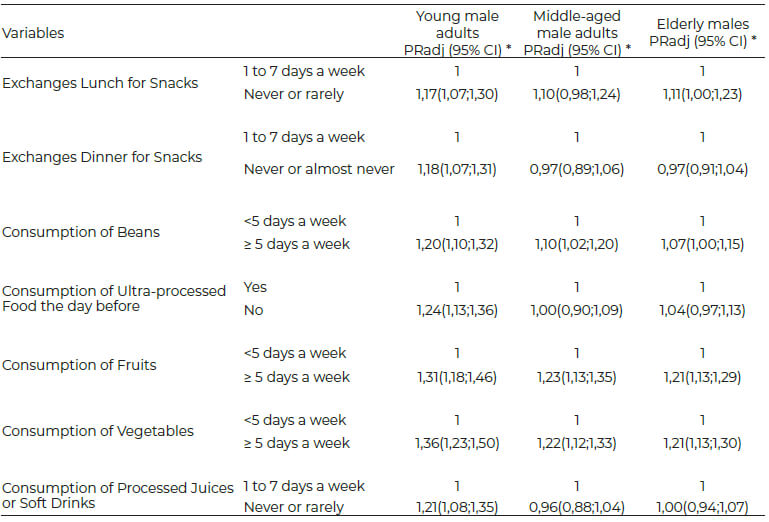
95% CI: 95% Confidence Interval.
* Adjustment of variables for gender, age, skin color, marital status, schooling, diabetes, hypertension, obesity, leisure-time physical activity, alcohol abuse, and tobacco use.
Regarding the prevalence of SPH with the number of healthy eating behaviors, a similar trend was observed in both genders, and the higher the number of healthy eating behaviors considered, in general, the higher the prevalence of positive SPH in all age groups (Figures 1 and 2).
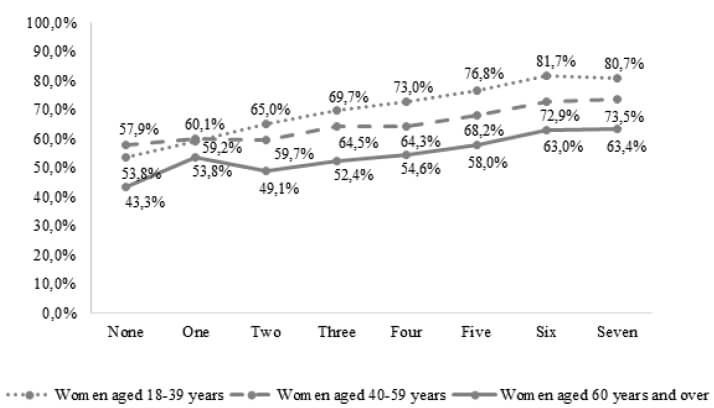
Figure 1: Prevalence of positive self-perceved health according to the score of healthy eating behaviors, in adult women aged 18 years or older living in Brazilian capitals. VIGITEL, Brazil, 2017. (n = 33219).
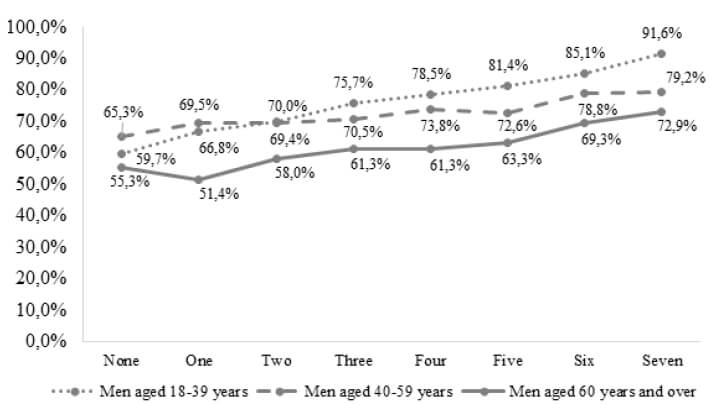
Figure 2: Prevalence of positive self-perceived health according to the score of healthy eating behaviors, in adult men aged 18 years or older living in Brazilian capitals. VIGITEL, Brazil, 2017. (n = 19412).
Discussion
Among the main findings of the study are: 1) The relationship between eating behaviors and positive SPH was more evident among young adults than between middle-aged and older adults; 2) All of the investigated eating behaviors showed at least one significant association with SPH, confirming the hypothesis of a positive relationship between healthy eating behavior and the best SPH ; 3) Of the eating patterns investigated, those related to the intake of fruits and vegetables showed a most evident relationship with positive SPH; 4) The higher the number of positive eating behaviors assumed, the higher the prevalence of positive SPH in both genders and all age groups.
This research observed a higher number of associations between the positive SPH relationship and eating behavior among the younger population, and similar results were found by Darviri et al. (23). These findings deserve special mention since there appears to be a higher awareness among younger people than among middle-aged and older individuals regarding health issues. Future studies could seek a more in-depth understanding of the issues related to eating habits by age group, including what each group considers healthy eating and its relationship with a better SPH. At least part of these results is attributable to the fact that younger individuals are more concerned with body aesthetics when compared to older individuals. For example, it would be worth investigating how many variables related to body image satisfaction can mediate the relationship between food eating patterns and self-perceived health. This study does not provide information on body image.
Of the dietary behaviors studied, the consumption of fruits and vegetables is the most strongly associated with a positive SPH. A similar relationship was found among Greeks by Darviri et al. (23) when relating five eating behaviors with SPH (consumption of meat, vegetables, fruits, legumes, and fish). Babo et al. (15), considered nine eating patterns (intake of red meat, fish, fruits, vegetables, water, percentage of carbohydrates, proteins, fats, and fibers in the diet) in older Portuguese adults, and by Hong & Peltzer, (27), who evaluated eight eating behaviors in Korean adolescents (breakfast, consumption of soft drinks, juices, caffeinated drinks, fast food, fruits, vegetables, and milk).
The strong relationship between positive SPH and regular consumption of fruits and vegetables is possibly explained by the high nutritional value of these foods and their role as regulators of the human body’s biological processes, given their high vitamins, minerals, and fiber content (31,32). It is worth mentioning that Brazilian health authorities encourage the intake of these foods through public policies (33,34).
Among the findings of this research, the association between "rarely exchanging lunch and dinner" with positive SPH in young adults of both genders is noteworthy. The frequent replacement of conventional meals (breakfast/lunch/dinner) for snacks and fast foods is related to poor health indicators such as high body fat, obesity, hypertension, hypercholesterolemia, and diabetes (35). In general, quick snacks tend to be low in micronutrients and have high-fat contents (35,36). A possible hypothesis that explains the association between making the eventual exchange of dinner for snacks with positive SPH in older women is that the energy needs in this group are lower when compared to the other groups studied, and possibly the foods consumed to replace dinner do not necessarily represent unhealthy foods, but only fewer calories.
This study found an association between regular consumption of beans in young adults of both genders and middle-aged adult men. It is still uncommon to associate this behavior with positive SPH. It is more common in the literature to associate health-related behaviors with the consumption of legumes and eggs (15,20). Beans are a legume of high nutritional value, rich in proteins, iron, and other micronutrients (37), and are present in the diet of many Brazilians (29). Studies have found associations between the regular intake of this food and keeping weight within the desired parameters and as well as the protection against various diseases (37,38).
An important finding in this study is the strong relationship observed between the number of healthy eating behaviors and the awareness of positive SPH. It applies for both genders and the three age groups investigated.
This study has some limitations, such as the cross-sectional design that does not allow to conclude regarding causality, and the non-presence of variables related to economic level or income (which can be minimized by having used schooling, which is a critical income/economic level proxy). In addition, the difficulty in accurately measuring food intake, given the complexity of this behavior, the lack of validity of some eating behaviors studied and its score, and the subjective nature of the SPH variable makes it problematic to accurately determine which aspects an individual considers when answering how they perceive their current health status.
The strengths of this research are the good statistical power to verify the associations and originality since few studies have invested in the association of several eating behaviors with positive SPH. The stratified analysis by age group allowed observing important specificities regarding the association of eating behaviors and SPH by age group.
Future research may include other dietary indicators and better understand what people understand as healthy and unhealthy foods. Longitudinal studies, which allow advancing concerning knowledge about the causality of the relationship between food and self-perceived health, would also be of great importance.
Conclusion
The study points out that healthy eating behaviors are associated with better SPH, and this relationship is more explicit in young adults with regular intake of fruits and vegetables. These findings rein force the importance of promoting healthy eating public policies.
Acknowledgments
Kretschmer AC was supported by the Coordination for the Improvement of Higher Education Personnel (CAPES) with a doctoral scholarship.
Conflict of interest
The authors declare no conflict of interest.
References
- Wu S, Wang R, Zhao Y, Ma X, Wu M, Yan X, He J. The relationship between self-rated health and objective health status: a population-based study. BMC Public Health. 2013; 13(320). https://doi.org/10.1186/1471-2458-13-320
- Falk H, Skoog I, Johansson L, Guerchet M, Mayston R, Hörder H, Prince M, Prina AM. Self-rated health and its association with mortality in older adults in China, India, and Latin America. Age Ageing. 2017; 46(6):932-39. https://doi.org/10.1093/ageing/afx126
- Schnittker J, Bacak V. The Increasing Predictive Validity of Self-Rated Health. Plos One. 2014; 9(1): e84933. https://doi.org/10.1371/journal.pone.0084933
- Szybalska A, Broczek K, Puzianowska-Kuznicka M, Slusarczyk P, Chudek J, Skalska A, Mossakowska M. Self-rated health and its association with all-cause mortality of older adults in Poland: The PolSenior project. Arch Gerontol Geriatr. 2018; 79:13-20. https://doi.org/10.1016/j.archger.2018.07.016
- Hua X, Lung TW, Woodward M, Salomon JA, Hamet P, Harrap SB, Mancia G, Poulter N, Chalmers J, Clarke PM. Self-rated health scores predict mortality among people with type 2 diabetes differently across three different country groupings: findings from the ADVANCE and ADVANCE-ON trials. Diabet Med. 2020. https://doi.org/10.1111/dme.14237
- Theme Filha MM, Szwarcwald CL, Souza Junior PRB. Measurements of reported morbidity and interrelationships with health dimensions. Rev. Saúde Pública. 2008; 42(1):73-81. https://doi.org/10.1590/S0034-89102008000100010
- Mavaddat N, Parker RA, Sanderson S, Mant J, Kinmonth AL. Relationship of Self-Rated Health with Fatal and Non-Fatal Outcomes in Cardiovascular Disease: A Systematic Review and Meta-Analysis. PLoS One. 2014; 9(7): e103509. https://doi.org/10.1371/journal.pone.0103509
- Osibogun O, Ogunmoroti O, Spatz ES, Burke GL, Michos ED. Is self-rated health associated with ideal cardiovascular health? The Multi-Ethnic Study of Atherosclerosis. Clin Cardiol. 2018;41(9):1154‐63. http://dx.doi.org/10.1002/clc.22995
- Wang A, Arah OA. Body Mass Index and Poor Self-Rated Health in 49 Low-Income and Middle-Income Countries, By Sex, 2002–2004. Prev Chronic Dis. 2015; 20(12):133. https://doi.org/10.5888/pcd12.150070
- Mcdaid O, Hanly MJ, Richardson K, Kee F, Kenny AR, Savva GM. The effect of multiple chronic conditions on self-rated health, disability, and quality of life among the older populations of Northern Ireland and the Republic of Ireland: a comparison of two nationally representative cross-sectional surveys. BMJ Open. 2013; 3(e002571):1-9. https://doi.org/10.1136/bmjopen-2013-002571
- Reichert FF, Loch MR, Capilheira MF. Autopercepcão de saúde em adolescentes, adultos e idosos. Cien Saude Colet. 2012;17(12):3353-3362. https://doi.org/10.1590/S1413-81232012001200020
- Jylha M, Guralnik JM, Ferrucci L, Jokela J, Heikkinen E. Is self-rated health comparable across cultures and genders? J Gerontol B Psychol Sci Soc Sci. 1998; 53(3): S144-52. https://doi.org/10.1093/geronb/53b.3.s144
- Baćak V, Ólafsdóttir S. Gender and validity of self-rated health in nineteen European countries. Scand. J. Public Health. 2017; 45(6): 647-653. https://doi.org/10.1177/1403494817717405
- Andrade GF, Loch MR, Silva AMR. Mudanças de comportamentos relacionados à saúde como preditores de mudanças na autopercepção de saúde: estudo longitudinal (2011-2015). Cad. Saúde Pública. 2019; 35(4):e00151418. https://doi.org/10.1590/0102-311x00151418
- Babo M, Poinhos R, Franchini B, Afonso C, Oliveira BMPM, Almeida MDV. The relationship between health self-perception, food consumption, and nutritional status among Portuguese older adults. Eur J Clin Ntr. 2019; 73(12):1613-1617. https://doi.org/10.1038/s41430-019-0473-2
- Machón M, Vergara I, Dorronsoro M, Vrotsou K, Larrañga I. Self-perceived health in functionally independent older people: associated factors. BMC Geriatr. 2016; 16(66). https://doi.org/10.1186/s12877-016-0239-9
- Saravia JC, Chau C. What factors are related to self-perceived health? The relationship between Sense of Coherence, behaviors, and health on Peruvian emerging adults, J. Health Soc. Behav. 2017; 9(2):111-16. https://doi.org/10.1016/j.jbhsi.2017.11.003
- Osera T, Awai M, Kobayashi M, Tsutie S, Kurihara N. Relationship between Self-Rated and Lifestyle and Food Habits in Japanese High School Students. Behav Sci. 2017; 7(4). https://doi.org/10.3390/bs7040071
- Câmara SG, Strelhow M. Self-Perceived Health among School-Aged Adolescents: a School-Based Study in Southern Brazil. Applied Research in Quality of Life. 2019; 14(3):603-615. https://doi.org/10.1007/s11482-018-9614-3
- Abuladze L, Kunder N, Lang K, Vaask S. Associations between self-rated health and health behaviour among older adults in Estonia: a cross-sectional analysis. BMJ Open. 2017;7(e013257):1-9. http://dx.doi.org/10.1136/bmjopen-2016-013257
- Meirelles AL, Xavier CC, Andrade ACDS, Friche AADL, Proietti FA, Caiaffa WT. Self-rated health in urban adults, perceptions of the physical and social environment, and reported comorbidities: The BH Health Study. Cad. Saúde Pública. 2015;31(Suppl1):120-135. https://doi.org/10.1590/0102-311X00076114
- Zarini GG, Vaccaro JA, Canossa Terris MA, Exebio JC, Tokayer L, Antwi J, Ajabshir S, Cheema A, Huffman FG. Lifestyle behaviors and self-rated health: the living for health program. J Environ Public Health. 2014. https://doi.org/10.1155/2014/315042
- Darviri C, Artemiadis AK, Tigani X, Alexopoulos EC. Lifestyle and self-rated health: a cross-sectional study of 3,601 citizens of Athens, Greece. BMC Public Health. 2011; 11(1). https://doi.org/10.1186/1471-2458-11-619
- Sodergren M, McNaughton SA, Salmon J, Ball K, Crawford DA. Associations between fruit and vegetable intake, leisure-time physical activity, sitting time and self-rated health among older adults: cross-sectional data from the WELL study. BMC Public Health. 2012; 25(12):551. https://doi.org/10.1186/1471-2458-12-551
- Goodwin DK, Knol LL, Eddy JM, Fitzhugh EC, Kendrick OW, Donahue RE. The Relationship between Self-Rated Health Status and the Overall Quality of Dietary Intake of US Adolescents. American Dietetic Association. 2006; 106(9):1450-3. https://doi.org/10.1016/j.jada.2006.06.011
- Collins CE, Young AF, Hodge A. Diet quality is associated with higher nutrient intake and self-rated health in mid-aged women. J Am Coll Nutr. 2008; 27(1):146-57. https://doi.org/10.1080/07315724.2008.10719686
- Hong S, Peltzer K. Dietary behaviour, psychological well-being and mental distress among adolescents in Korea. Child Adolesc Psychiatry Ment Health. 2017; 11(56). https://doi.org/10.1186/s13034-017-0194-z
- Jiménez-Redondo S, Beltrán MB, Gavidia BJ, Guzmán ML, Gómez-Pavón J, Cuadrado VC. Influence of nutritional status on health-related quality of life of non-institutionalized older people. J Nutr Health Aging. 2014; 18(4):359-64. https://doi.org/10.1007/s12603-013-0416-x
- Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância de Doenças e Agravos não Transmissíveis e Promoção da Saúde. Vigitel. Brasil 2017: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Secretaria de Vigilância em Saúde, Departamento de Vigilância de Doenças e Agravos não Transmissíveis e Promoção da Saúde. Brasília: Ministério da Saúde; 2018.
- World Health Organization. Ageing and health. [Internet]. 2021 [accessed 2022 April 16th]. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health
- Slavin JL, Lloyd B. Health benefits of fruits and vegetables. Adv Nutr. 2012; 3(4):506-16. https://doi.org/10.3945/an.112.002154
- Wallace TC, Bailey RL, Blumberg JB, Burton-Freeman B, Oliver Ch, Crowe-White KM et al. Fruits, vegetables, and health: A comprehensive narrative, umbrella review of the science and recommendations for enhanced public policy to improve intake. Crit. Rev. Food Sci. Nutr. 2019; 60(13):2174-2211. https://doi.org/10.1080/10408398.2019.1632258
- Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Política Nacional de Alimentação e Nutrição. Ministério da Saúde, Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Brasília: Ministério da Saúde, 2013.
- Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Secretaria de Atenção à Saúde. Política Nacional de Promoção da Saúde. Ministério da Saúde, Secretaria de Vigilância em Saúde, Secretaria de Atenção à Saúde. – 3. ed. – Brasília: Ministério da Saúde, 2010.
- De Vogli R, Kouvonen A, Gimeno D. The influence of market deregulation on fast food consumption and body mass index: A cross-national time series analysis. Bull. World Health Organ. 2014;92:99–107. https://doi.org/10.2471/BLT.13.120287
- Pereira MA, Kartashov AI, Ebbeling CB, Van Horn L, Slattery ML, Jacobs DR, Ludwig DS. Fast-food habits, weight gain, and insulin resistance (the CARDIA study): 15-year prospective analysis. Lancet. 2005;365:36–42. https://doi.org/10.1016/S0140-6736(04)17663-0
- Messina V. Nutritional and health benefits of dried beans. Am J Clin Nutr. 2014; 100 (suppl. 1): 437S-442S. https://doi.org/10.3945/ajcn.113.071472
- Papanikolaou Y, Fulgoni VL. Bean consumption is associated with greater nutrient intake, reduced systolic blood pressure, lower body weight, and a smaller waist circumference in adults: results from the National Health and Nutrition Examination Survey 1999-2002. J Am Coll Nutr. 2008; 27(5):569-576. https://doi.org/10.1080/07315724.2008.10719740