Introduction
In December 2019, in the city of Wuhan, province of Hubei, the first cases of the coronavirus disease (COVID-19) caused by the SARS-CoV-2 virus were reported. Despite of the efforts to contain the COVID-19 outbreak, the World Health Organisation (WHO) declared COVID-19 a pandemic on March 11th, 2020 (1,2). With the announcement of the pandemic, countries started to take containment and mitigation measures, emphasizing social distancing and quarantine (3). These contingency measurements are expected to have a great economic impact in high, middle- and low-income countries (4).
According to the Global Report on Food Crises 2025, more than 295 million people across 53 countries and territories experienced acute food insecurity in 2024, an increase of 13.7 million over the previous year (5). A person is considered food insecure when they lack regular access to sufficient, safe, and nutritious food to support normal growth, development, and an active, healthy life. In this regard, the basic pillars of food security must be considered: availability, access, biological utilization, and the stability of these three, as established at the FAO World Food Summit (1996) (6). This may be due to the unavailability of food and/or lack of resources to obtain food. FI can be experienced at different levels of severity (7).
Indeed, FI levels will differ within regions, with expectations that women and children from low and medium-income countries would be the most affected by the indirect effects of the COVID-19 crisis (7). In addition, there has been growing concern about the impact of COVID-19 on household food insecurity (8,9). Disruptions caused by the pandemic have the potential to influence the pillars of food security, including availability, access, utilization and stability (10). The COVID-19 pandemic may directly influence FI by disrupting food systems (such as primary food production, production stability, processing, food stocks and marketing) and indirectly through the impact of quarantines on households (reduced income, physical and economic access to food) (11).
It has been estimated that the effects of FI, as well as the decrease in essential services such as child healthcare, could result in the deaths of 42,240 children under five years old and 2,030 additional maternal deaths per month worldwide (7).
Severity will depend, among other factors, on people's socioeconomic status, levels of FI being the highest among people with low socioeconomic level and/ or education (8). This is especially relevant in Latin America, a region characterized by high levels of social inequality (9). Among the Latin American region, Chile is one of the countries with high levels of social inequality (12). Although access to higher education in Chile has increased eight-fold in the lowest deprivation quintile since the 90s, the education gap persists when comparing those in the lowest and highest deprivation quintile. According to the National Socioeconomic Characterization Survey (CASEN), food insecurity increased during the pandemic from 13.6% in 2017 to 19.6% in 2020, followed by a slight decline to 19.5%. (2022) (13). Considering the existing inequality and the direct and indirect effect of the COVID-19 pandemic in Chile, and the lack of knowledge about the prioritization of food purchases in the basic food basket of Chileans during this period; Given the existing inequality and the direct and indirect effects of the COVID-19 pandemic in Chile, along with the limited understanding of how food purchases within the basic basket were prioritized during this period, the need arises for more detailed investigation of this issue. Although a recent study by the authors (14). explored the prioritization of certain foods, the factors influencing such prioritization remain unclear. Therefore, it is crucial to understand how sociodemographic factors are associated with food insecurity in Chile during the ongoing COVID-19 pandemic. Therefore, the aim of this study was to investigate what socio-demographic factors are associated with food insecurity and what food groups are prioritized by individuals with FI during the COVID-19 pandemic in the Chilean population.
Material and methods
Study design and Subjects
This cross-sectional study included individuals aged 18 years or older who were Chilean residents and had lived in Chile for at least the past five years. Participants were invited to take part in the study through email and social media platforms such as Twitter, Facebook, LinkedIn, and Instagram. Individuals unable to provide informed consent were excluded from the study. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Scientific Ethics Committee of the Pontificia Universidad Católica de Chile (number: 200327001).
Procedures
An online questionnaire designed in Google form was sent once to the participants via email between April 13th and May 17th of 2020. The questionnaire included a total of 48 questions regarding socio-demographic factors (10 questions), purchasing priority of some selected food products (26 questions), and household food security (12 questions). Food security was assessed using the Household Food Security Scale validated in Spanish by Lorenzana (15,16). The scale comprises 12 items related to the availability of money to buy food, the reduction or skipping of meals due to the lack of money and the experience of hunger by some of the household members during the last six months. The rate of occurrence of each item was codified as follows: three times correspond to "always"; twice corresponds to "sometimes"; once corresponds to "rarely" and zero to "never". The use of this codification made it possible to generate a FI score ranging from 0 to 36 points; households were classified in four categories: 0 points mean "secure"; 1-12 points mean "mild food insecurity"; 13-24 points mean "food insecurity with moderate hunger", and 25 or more points mean "food insecurity with severe hunger" (15). To determinate the prioritization of purchase, people answered for different food items if they had low, middle, high prioritization or did not buy the product. Foods that were included are part of the basic food basket of Chileans, which includes bread and cereals, meats, fish, dairy products, eggs, oils, fruits, vegetables, legumes, potatoes, sugar, sweetened beverages, wine, meals outside the home, as well as dried fruits and nuts and cured meats (17).
Statistical analysis
Continuous data were expressed in mean ± SD, qualitative values in frequency and percentages. For the association tests, researchers used the Chi2 or Fisher test. To determine if the main socio-demographic factors were associated with FI, we used logistic regression analysis, where FI was the outcome (coded as 0 = food security and 1= food insecurity (which included low, moderate and severe food insecurity)). Variables included in the model were sex, education, socioeconomic level, nutritional status, occupation, children, and older people in the household. To determine what food groups were prioritized among individuals with FI and those without FI, logistic regression was performed where food prioritization was the outcome, and FI was the exposure. For this analysis, each food item was coded as a binary variable, with 0 = low prioritization (when the answer was low prioritization or no purchase) and 1 = high prioritization (when the answer was middle or high prioritization). Using stepwise methods, the analysis was adjusted by age, sex, socioeconomic level, level of education, weeks in quarantine and nutritional status. Results are presented as odds ratios (OR) with their respective 95 % CI. The statistical package R version 4.0.3 was used to perform all analyses. A p value of <0.05 was considered significant.
Results
Table 1 shows the characteristics of the population studied. A total of 1,114 people answered the survey, 87.8% were women, 53.2% had been in quarantine, and more than 60.2% had higher education (complete or incomplete). Of the responders, 32.3% reported living with a child, and 35.6% of the respondents reported living with an older adult. Regarding employment, 13.1% of the participants were unemployed, and 36.1% were dependent workers. For food security assessment, 61.7% were classified as food-secure, 32.3% mildly food-insecure, 5.7% moderately food-insecure and 0.4% severely food-insecure.
Table 1. General characteristics of the sample by sex and food insecurity status
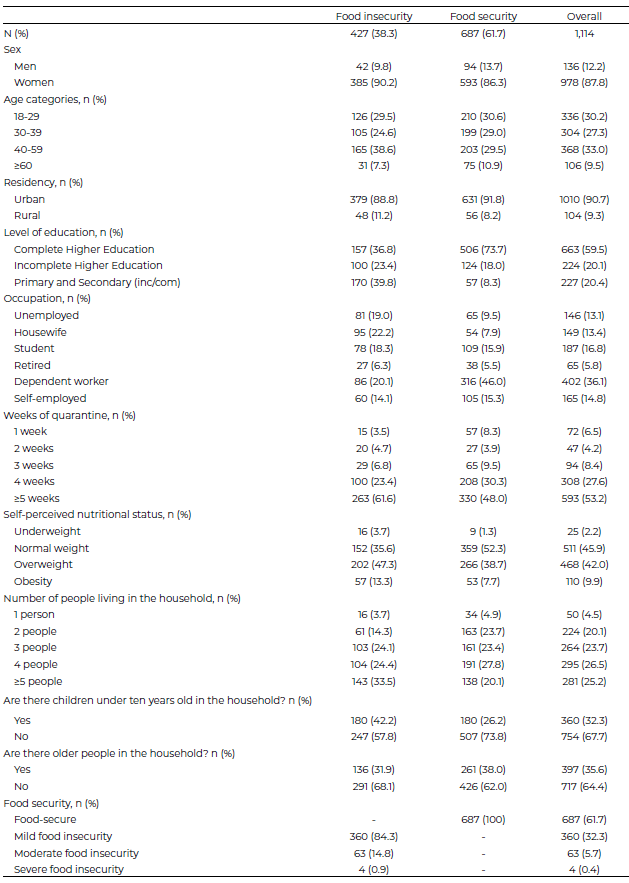
Data is presented as frequency and percentage.
Table 2 shows the association of FI by different socio-demographic factors. Those with secondary and university education were 79% and 59% less likely to experience FI, respectively, compared to individuals with primary education. Similarly, favorable associations were found for those with middle and high socioeconomic levels compare to those with low. When it came to occupation status, those who were independent workers, retired, student, unemployed and housewives were between 1.4- and 3.4-times more likely to experience FI. Individuals who live with children were 1.6-times more likely to experience FI, while those living with older adults were 28% less likely. There were also lower odds of FI for those who were underweight, who were 68% less likely to experience FI compared with those who perceived weight themselves as having a normal bodyweight. No differences were found across age group, sex, and place of residency.
Table 2. Food insecurity by sociodemographic variables.
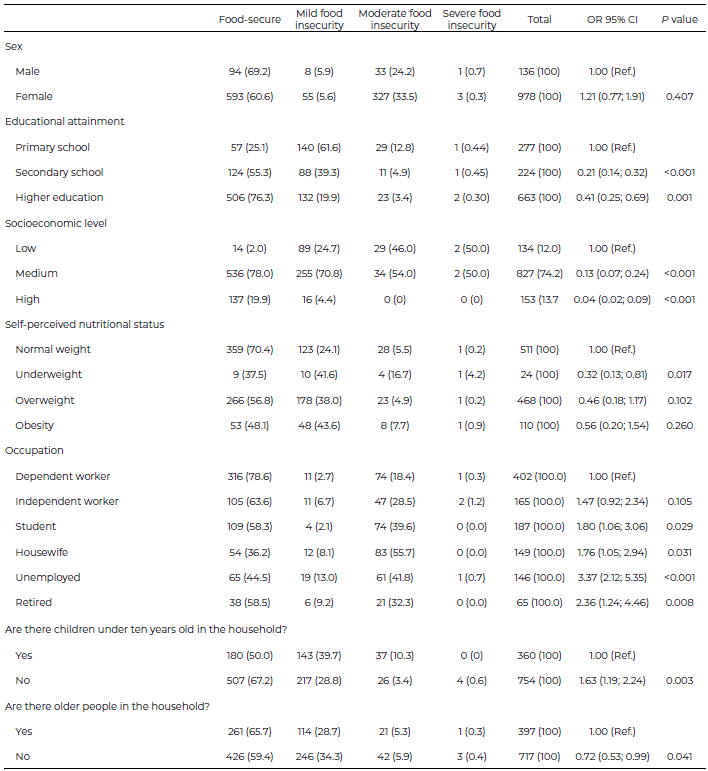
Data is presented as frequency and percentage and odds Ratio (OR) for food insecurity with their 95% confidence interval (CI). Variables included in the model were sex, education, socioeconomic level, nutritional status, occupation, children, and older people in the household. The reference group was people without food insecurity denoted as 1.00 (Ref.).
The associations between food groups preference and FI are shown in Figure 1. Participants with FI, compared to those without, were 1.7-times more likely to prioritize the purchase of sugar (OR;1.71: CI95% 1.30-2.24), 52% more likely to prioritize rice & pasta (OR;1.52: CI95% 1.06-2.18), 42% more likely to prioritize sausages (OR;1.42: CI95% 1.07-1.89). While in contrast, meat, cookies, bread, chocolates, fries, alcohol, fruits and vegetables were between 32% and 67% less likely to be prioritized among individuals experiencing FI.
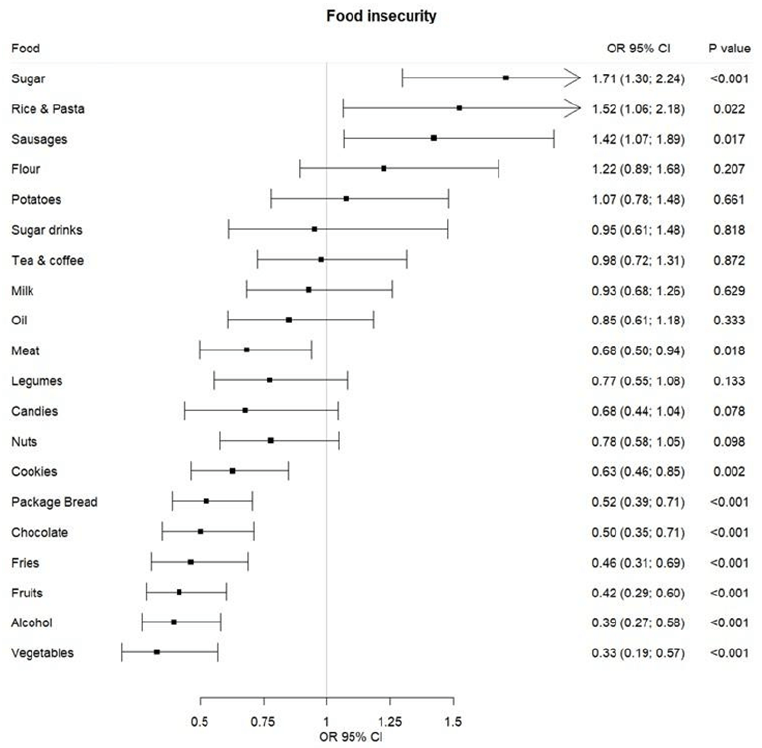
Data are presented in the odds ratio with 95% confidence intervals. The reference group was low prioritized of food group. Model was adjusted by age, sex, socioeconomic level, level education, weeks in quarantine and nutritional status.
Figure 1. Association of food purchase prioritization with food insecurity
Discussion
The results show that having a child under ten years old, being unemployed, being a housewife, and giving a high priority to the purchase of sugar, rice and pasta, and sausages are associated with FI.
At the time of the present study, Chile and the world are undergoing a sanitary crisis by COVID-19; this situation has negatively influenced the health and the food security of individuals and their households (18) and even more so if they are quarantined. In the present research, participants in quarantined areas duplicated their FI level by the fifth week. Other adverse consequences of the crisis situation are reflected in the food system, incomes and food consumption. The COVID-19 crisis has brought negative impacts on the economy, income generation and employment. This situation can be seen in this research. In Chile, as in the rest of Latin America, there is a large number of people working informally, so confinements directly affect income and the ability to buy fresh food (19).
Poverty, low incomes and low SEL are predictors of FI [20]. In Chile, The National Survey of Food Consumption showed a lower consumption of dairy products, fruits and vegetables, red meats, fish and seafood among the low socioeconomic level (SEL) (21). The WHO considers that a healthy diet must include enough fruits and vegetables, nuts, seeds, whole grains and minimal amounts of processed meats, free sugars, saturated fats, trans fats and salt (22). Clearly, following these recommendations requires a greater investment in economic terms and better purchase decisions. Populations with low incomes do not follow these patterns and tend to choose less expensive, highly caloric, low-nutrient-dense foods such as sugar, rice or sausages; this information is consistent with the findings of this study and with data reported in other studies (23). Education is undoubtedly a protective factor; however, the economic downturn triggered by the COVID-19 pandemic further constrained households’ ability to access nutritious foods. While many were aware of the need to adopt healthier diets, financial limitations and restricted access prevented them from doing so, particularly among low-income groups, for whom the pandemic represented a double burden: pre-existing vulnerability compounded by the health and economic crisis. Food prioritization among low-income populations is therefore shaped by economic constraints, leading to the purchase of inexpensive, calorie-dense but nutrient-poor foods a mechanism that helps explain the growing association between poverty and overweight or obesity.
It is possible that people who are experiencing FI, by prioritizing foods such as flour (to make bread and other preparations with it), pasta/ rice, sugar and oil, can present lower intakes of protein, vitamins especially A, C, B12, minerals such as calcium and zinc among others and a lower intake of antioxidants and dietary fibre. For example, in our study, we observed a low prioritization of buying fruits and vegetables. These two food groups are good sources of water, antioxidants and fibre, all of which play a role in the control of hypertension, diabetes and weight gain. Some of the most important risk factors in complications of COVID-19 (24). On the other hand, it is observed that people with FI have a greater prioritization in the purchase of sugar, rice, pasta and sausages, foods with low or no nutrient intake, but which generate satiety. This result is similar to another study published in Latin America (25). In addition, stressors specific to confinement were added to the classic factors influencing food purchases (26).
In this investigation, greater levels of FI were found among those respondents that according to their perception were underweight or obese. Poverty is associated with FI in Latin America and the Caribbean, while in Eastern Europe, Central and Eastern Asia, there is evidence of an increasing occurrence of overweight and obesity among the poor population. This is in opposition to the trend observed in Sub-Saharan Africa and South Asia, where the greatest prevalence was observed among the higher-income population (27). Other studies have also reported an association between overweight and low incomes (28,29). Obesity rates continue to rise worldwide as well as in Chile, and the crisis is likely to increase malnutrition in all its forms especially among vulnerable groups (30). Moreover, several studies have demonstrated an association between poverty and a higher prevalence of overweight and obesity (31,32). This relationship may be explained by multiple mechanisms, including limited health literacy, restricted access to healthy food options, lack of safe environments for physical activity, lower utilization of healthcare services, and elevated levels of chronic stress (33).
Another factor associated with FI is family composition (19). Several studies have revealed that the presence of children in the household is associated with lower food security (34-36), as well as families with members under 18 years old (37). Similar findings were reported at the national level; families with children and adolescents had the greatest levels of FI (20). In Australia, the presence of children in the household was associated with lower fruit consumption; it is likely that food choices are made according to children's preferences, and fast food and meals rich in fats and sugars are prioritized. Lower incomes are associated with low educational attainment (38) and FI (39). In urban areas, the association between educationallevelandfoodsecurityismediated by its relationship with employment, income and decision making, directly impacting in the availability of foods, access to them and their consumption. In Chile, FI level were double when a comparison of the illiteracy or literacy of the head of the household was made (19). In this study, participants with higher education had a lower risk of FI.
Among the strategies to improve nutrition and reduce FI is nutrition education, and there is extensive literature that shows that it can generate positive changes in nutrition, including the use of telemedicine (40), which can become an important educational tool during and after the pandemic (41,42).
One of the main limitations of this study is that it is not based on a representative sample. In particular, there is a high proportion of women and individuals with higher education, even though a large part of the Chilean population has only completed secondary education. This composition may influence the interpretation of the findings, as both factors are associated with distinct behavioral patterns, resource access, and health outcomes compared to the general population. In a context of pronounced social inequality, as observed in this study, the overrepresentation of these groups may reflect greater awareness or access to healthy practices, as well as reduced exposure to certain structural barriers. However, it also limits the generalizability of the results to populations with lower educational attainment or to men, who may face different conditions and social determinants that could alter the observed associations. In addition, the use of the STEPwise method for variable selection in regression modeling is discouraged in modern statistics, as results can vary with small changes in the data and it does not necessarily identify the most parsimonious or best-fitting model. Finally, the cross-sectional design precludes causal inference, though it does allow for the identification of associations. Among the strengths, we may highlight the use of a validated survey. Therefore, it is possible to compare the data with other similar studies performed in the region.
Conclusions
Socioeconomic factors are critical determinants of FI during the COVID-19 crisis. Evidence shows that FI was particularly severe in low-income settings, a situation further aggravated by the economic downturn caused by quarantine measures, which reduced income opportunities and shifted household purchasing decisions toward highly caloric but nutrient-poor foods. The problem was especially pronounced in households with children under 10 years of age, a group requiring special attention due to their heightened vulnerability in terms of nutrition, health, and care. The coexistence of multiple forms of malnutrition alongside FI highlights the urgent need for dual-purpose interventions that simultaneously address child nutrition, diet quality, the food environment, and the broader socioeconomic determinants of health.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
1st competition to support scientific publication, Department of Nutrition and Dietetics, School of Health Sciences, Pontificia Universidad Católica de Chile, 2025
References
- Lake MA. What we know so far: COVID-19 current clinical knowledge and research. Clinical Medicine, Journal of the Royal College of Physicians of London. 2020. https://doi.org/10.7861/clinmed.2019-coron
- World Health Organization. COVID-19 Situation Report. World Heal Organ. 2020;
- PoliMap – COVID-19. https://polimap.org/
- CEPAL. Coyuntura Laboral en América Latina y el Caribe. El trabajo en tiempos de pandemia: desafíos frente a la enfermedad por coronavirus (COVID-19). 2020. https://hdl.handle.net/11362/45557
- Acute Food Insecurity and Malnutrition Rose for Sixth Consecutive Year in World’s Most Fragile Regions.World Food Program, USA https://www.wfpusa.org/news/acute-hunger-malnutrition-rose-sixth-consecutive-year/?utm_source=chatgpt.com
- World Food Summit. Rome Declaration on World Food Security [Internet]. [cited 2025 september 22]. https://www.fao.org/4/w3613e/w3613e00.htm
- Health TLG. Food insecurity will be the sting in the tail of COVID-19. The Lancet Global Health . 2020;8:e737. https://pubmed.ncbi.nlm.nih.gov/32446335/
- Mutisya M, Ngware MW, Kabiru CW, Kandala N. The effect of education on household food security in two informal urban settlements in Kenya: a longitudinal analysis. Food Sec. 2016;8:743-756. https://link.springer.com/article/10.1007/s12571-016-0589-3#:~:text=Using%20longitudinal%20 data%20collected%20between,security%20among%20poor%20urban%20households.&text=The%20probability%-20of%20being%20food,schooling%20for%20a%20given%20 household.
- Inequalities in life expectancy in six large Latin American cities from the SALURBAL study: an ecological analysis - The Lancet Planet Health [Internet]. [cited 2020 Jun 12]. Available from: https://www.thelancet.com/journals/lanplh/article/PIIS2542-5196(19)30235-9/fulltext (accessed September 2020).
- Cable J, Jaykus LA, Hoelzer K, Newton J, Torero M. The impact of COVID-19 on food systems, safety, and security—a symposium report. Ann N Y Acad Sci. 2021;1484(1):3–8. https://doi.org/10.1111/nyas.14482
- Laborde D, Martin W, Swinnen J, Vos R. COVID-19 risks to global food security. Science. 2020;369(6503):500–502. https://doi.org/10.1126/science.abc4765
- Parro F, Reyes L. The rise and fall of income inequality in Chile. Lat Am Econ Rev. 2017;26:3. https://doi.org/10.1007/s40503-017-0040-y
- Evolución de los indicadores de inseguridad alimentaria antes, durante y después de la pandemia. ENCUESTA CASEN 2017-2022. [Internet]. [cited 2025 september 22]. https://observatorio.ministeriodesarrollosocial.gob.cl/storage/docs/casen/2022/Resultados_Inseguridad_Alimentaria_Casen_2022_dic2024.pdf
- Prada GE, Durán-Agüero S, Moya-Osorio JL. [Confinement and food insecurity during the COVID-19 pandemic in Chile]. Rev Chil Nutr. 2021;48(5): 678-686. http://doi.org/10.4067/S0717-75182021000500678
- Lorenzana Dellohain P, Sanjur D. La adaptación y validación de una escala de seguridad alimentaria en una comunidad de Caracas, Venezuela. Arch Latinoam Nutr. 2000;50(4). https://www.alanrevista.org/ediciones/2000/4/art-3
- Álvarez MC, Estrada A, Montoya EC, Melgar-Quiñónez H. Validación escala la Seguridad Alimentaria doméstica en Antioquia, Colombia. Salud Publica Mex. 2006;48(6):474–481. http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S0036-36342006000600005
- Ministerio de Desarrollo Social y Familia. Observatorio Social - Ministerio de Desarrollo Social y Familia [Internet]. [cited 2021 May 23]. Available from: http://observatorio.ministeriodesarrollosocial.gob.cl/nueva-serie-cba-2021
- Organización Internacional del Trabajo (OIT). Panorama Laboral 2020, América Latina y el Caribe. 2020.
- CEPAL. El desafío social en tiempos del COVID-19 | Publicación | Comisión Económica para América Latina y el Caribe [Internet]. 2020 [cited 2023 May 22]. Available from: https://www.cepal.org/es/publicaciones/45527-desafio-social-tiempos-covid-19
- Novoa-Sanzana S, Moya-Osorio J, Morejón Terán Y, Ríos-Castillo I, Becerra Granados LM, Prada Gómez G, et al. Food insecurity and sociodemographic factors in Latin America during the COVID-19 pandemic. Rev Panam Salud Publica. 2024;48:e21. https://doi.org/10.26633/rpsp.2024.21
- Universidad de Chile. Encuesta Nacional de Consumo Alimentario en Chile. 2010. Available from: http://web.minsal.cl/sites/default/files/ENCA-INFORME_FINAL.pdf (accessed September 2020).
- WHO. Healthy diet [Internet]. [cited 2021 May 22]. Available from: https://www.who.int/news-room/fact-sheets/detail/healthy-diet
- Wiggins S, Keats S. The rising cost of a healthy diet: changing relative prices of foods in high-income and emerging economies | odi.org [Internet]. 2015 [cited 2021 May 22]. Available from: https://odi.org/en/publications/the-rising-cost-of-a-healthy-diet-changing-relative-prices-of-foods-in-high-income-and-emerging-economies/
- Ramphul K, Lohana P, Ramphul Y, Park Y, Mejias S, Dhillon BK, et al. Hypertension, diabetes mellitus, and cerebrovascular disease predispose to a more severe outcome of COVID-19. Arch Med Sci Atheroscler Dis. 2021;6: e30-e39. https://doi.org/10.5114/amsad.2021.105255
- Quezada-Acuña L, Duran-Aguero S, Moya-Osorio J, Morejon-Terán Y, Ocampo L, Becerra-Granados L, et al. Food Purchase Prioritization During the COVID-19 Pandemic in Latin America. J Hunger Environ Nutr. 2024:19(6), 999–1013. https://doi.org/10.1080/19320248.2023.2232321
- Quezada-Acuña L, Parra-Soto S, Durán-Agüero S, Morejón-Terán Y, Pérez-Ocampo L, Becerra-Granados LM, et al. Stress factors and food purchase prioritization during the pandemic of coronavirus disease 2019. Clin Nutr ESPEN. 2024;61:145-150. https://doi.org/10.1016/j.clnesp.2024.03.001
- Popkin BM, Corvalan C, Grummer-Strawn LM. Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet. 2020;395(10217):65–74. https://doi.org/10.1016/s0140-6736(19)32497-3
- Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev. 2012;70(1):3–21. https://doi.org/10.1111/j.1753-4887.2011.00456.x
- Prada Gómez GE, Gutierrez MM, Angarita A. [Association between socioeconomic factors and body mass index among low-income preschoolers from an educational institution of Floridablanca, Colombia]. Rev Chil Nutr . 2015;42(4):337–344. http://doi.org/10.4067/S0717-75182015000400003.
- INE. Instituto Nacional de Estadísticas. Memoria. CENSO 2017 MEMORIA 2018 https://www.censo2017.cl/memoria/descargas/memoria/libro_memoria_censal_2017_final.pdf
- Inoue K, Seeman TE, Nianogo R, Okubo Y. The effect of poverty on the relationship between household education levels and obesity in U.S. children and adolescents: an observational study. Lancet Reg Health Am. 2023;25:100565. doi: 10.1016/j.lana.2023.100565.
- Sadhu R, Souza M, Borges C. The effect of food insecurity on the prevalence of adult obesity in New Jersey counties, Eur J Public Health. 2020;30(Issue Supplement_5):ckaa166.231. https://doi.org/10.1093/eurpub/ckaa166.231
- Lobstein T, Neveux M, Brown T, Chai LK, Collins CE, Ells LJ, Nowicka P; STOP project consortium. Social disparities in obesity treatment for children age 3-10 years: A systematic review. Obes Rev. 2021;22(2):e13153. doi: 10.1111/obr.13153.
- Harris DE, Aboueissa AM, Walter K, Bampton M. Predictors of Food Insecurity in Lewiston, Maine: A Community-Level Analysis. J Hunger Environ Nutr, 2014; 9:96-112. http://doi.org/10.1080/19320248.2013.840549
- Furness BW, Simon PA, Wold CM, Asarian-Anderson J. Prevalence and predictors of food insecurity among low-income households in Los Angeles County. Public Health Nutr. 2004; 7:791-794. https://doi.org/10.1079/phn2004608
- Lamidi EO. Household composition and experiences of food insecurity in Nigeria: the role of social capital, education, and time use. Food Sec. 2019;11(1):201–218. https://doi.org/10.1007/s12571-019-00886-2
- Tarasuk V, Fafard St-Germain AA, Mitchell A. Geographic and socio-demographic predictors of household food insecurity in Canada, 2011-12. BMC Public Health. 2019; 19:12. https://doi.org/10.1186/s12889-018-6344-2
- Seivwright AN, Callis Z, Flatau P. Food insecurity and socioeconomic disadvantage in Australia. Int J Environ Res Public Health. 2020;17(2):559. https://doi.org/10.3390/ijerph17020559.
- Faye O, Baschieri A, Falkingham J, Muindi K. Hunger and food insecurity in Nairobi’s slums: An assessment using IRT models. J Urban Heal. 2011;88: suppl 2 (Suppl. 2):235-255. https://doi.org/10.1007/s11524-010-9521-x
- Singh RH, Pringle T, Kenneson A. The Use of Telemedicine and Other Strategies by Registered Dietitians for the Medical Nutrition Therapy of Patients With Inherited Metabolic Disorders During the COVID-19 Pandemic. Front Nutr. 2021;8:637868. https://doi.org/10.3389/fnut.2021.637868.
- Neves FJ, Tomita LY, Liu ASLW, Andreoni S, Ramos LR. Educational interventions on nutrition among older adults: A systematic review and meta-analysis of randomized clinical trials. Maturitas. 2020;136:13–21. https://doi.org/10.1016/j.maturitas.2020.03.
- Li X, Huang Y, Yin R, Pan C, Cai Y, Wang Z. Visualized nutrition education and dietary behavioral change: A systematic review and meta-analysis. Crit Rev Food Sci Nutr. 2019;59(12):1976–1985. https://doi.org/10.1080/10408398.2018.1469466
