Introduction
Community Health Workers (CHW) are the professionals responsible for enabling prevention and health promotion, identifying health problems in certain spaces and idealizing clinical and sanitary interventions that are effective and effective in solving the problem (1,2). Having regard to its role, in addition to promotion, taking care of one’s own health is essential, so a healthy and appropriate diet, together with the strengthening of the immune system, is of paramount importance for the prevention of various infections, role in the treatment and rehabilitation of sick patients (3,4).
The CHW face in daily life several challenges, because they are the target of great demand of the population, which can trigger situations of extreme psychological have little time and consequently difficulty to plan healthy eating habits (5,6). In addition, Moreover, evidence indicates that chronic stress and lifestyle changes are associated with alterations in dietary patterns among the population, often leading to increased consumption of ultra-processed foods — a behavior that tends to persist even after the reduction of stressors (7,8).
The eating habits of health professionals, including ACS, often do not reflect the practices that they themselves guide the population (9). This contradiction may be related to poor working conditions, long hours, emotional overload and the absence of institutional policies aimed at self-care of workers (10).
This study aims to analyze the food consumption of community health agents (CHW) in the northern region of Minas Gerais.
Materials and methods
This research is part of the base project entitled "Working conditions and health of community health workers in the north of Minas Gerais". This was a cross-sectional study conducted with the CHW population of the Family Health Strategies (FHS) municipalities located in the northern region of Minas Gerais. The definition of the sample size took into account the following parameters: estimated prevalence of 50% (which provides the largest sample size), 95% confidence level and margin of error of 4%, with correction for finite population. Correction was performed for the design effect, adopting Deff = 2.0 and to compensate for possible non-responses and losses an increase of 12% was established. The minimum sample size of n = 1167 CHW was estimated, being n1 = 567 (48.6%) agents of the host municipalities and n2 = 600 (51.4%) of the other municipalities in the north of Minas Gerais.
The inclusion criterion used for the CHWs to participate in the study was to be registered in the National Registry of Health Facilities (CNES), and the non-inclusion criteria were to be on sick leave or on vacation, to be away or not accept to participate in the study. Data collection was conducted online between July and August 2020, through self-administered questionnaires (11). The questionnaire was made available to research participants through the WhatsApp messaging application, using the Google Forms system.
As regards the assessment of the ACS diet, the following items were used: frequency of ingestion of vegetables, fruits, snacks and processed/ultra-processed foods during the week (1 to 2 days a week, 3 to 4 days a week, 5 to 6 days a week, every day, almost never, ever). Food consumption was measured using items adapted from the questionnaire of the Chronic Disease Risk and Protective Factors Surveillance System (Vigitel) (11). Additionally, changes in eating habits during the pandemic were assessed (reduce a lot, reduce a little, stay the same, don't change, increase a little, increase a lot). In this study, the outcome variable was defined as the increase in the consumption of unhealthy foods (snacks and processed/ultra-processed foods) and the reduction in the consumption of healthy foods (vegetables, fruits) during the pandemic.
For the evaluation of sociodemographic factors, the following variables were considered: identification, sex (female or male), date of birth, schooling (elementary, incompletehighschool, completehighschool, incomplete higher education, complete higher education), family income (kept the same income, income decreased, income increased), number of people in the household during social isolation (kept the same number of people, decreased the number of people, increased the number of people), number of rooms in the household, marital status (single, divorced/separated/widowed, married/ stable union) and skin color (white, black, yellow, brown or indigenous).
To evaluate the practice of physical activity, we applied the International Physical Activity Questionnaire (IPAQ), a widely used tool recommended by the World Health Organization and validated for the Brazilian population (12). This instrument allows estimating the level of physical activity in adults based on the duration, intensity, and frequency of activities performed during the week preceding the interview. For analysis, the participants were classified into two categories: inactive or insufficiently active when accumulating less than 150 minutes of physical activity per week, and active when engaging in 150 minutes or more within the same period.
Pearson’s chi-square test was used in the bivariate analysis to evaluate factors associated with food consumption. The magnitude of the association between dependent and independent variables was assessed by the crude and adjusted Prevalence Ratio (PR), with their respective 95% confidence intervals (CI-95%). For the construction of the models, the backward criterion was used, with the removal of the variables from the model one by one, according to the p-value. For the permanence of the variables in the final model, a significance level of 5% was considered. To evaluate the possible factors associated with food consumption, the Poisson model with robust variances was used. The Deviance test was used to evaluate the quality of the final model. The data obtained were analyzed by the computer program Statistical Package for the Social Sciences (SPSS®) for Windows®, version 20.0.
The study project was approved by the Research Ethics Committee of the State University of Montes Claros (CEP/Unimontes): Opinion n. 2,425,756, issued on December 8, 2017. The Informed Consent Form was signed by the CHW as a precondition for data collection.
Results
The study included 1,220 Community Health Workers, most participants were women (85.1%) and under 40 years of age (71.1%), with up to 11 years of schooling (67%). More than half had over five years of professional experience (53.2%) and were employed under CLT-type contracts (60.6%). Regarding lifestyle characteristics, 50.6% did not engage in physical activity. The other sociodemographic characteristics, working conditions, health and life habits are described in Table 1 and Table 2.
Table 1. Unhealthy food consumption among community health agents, according to sociodemographic variables and working in the north of Minas Gerais, 2020.
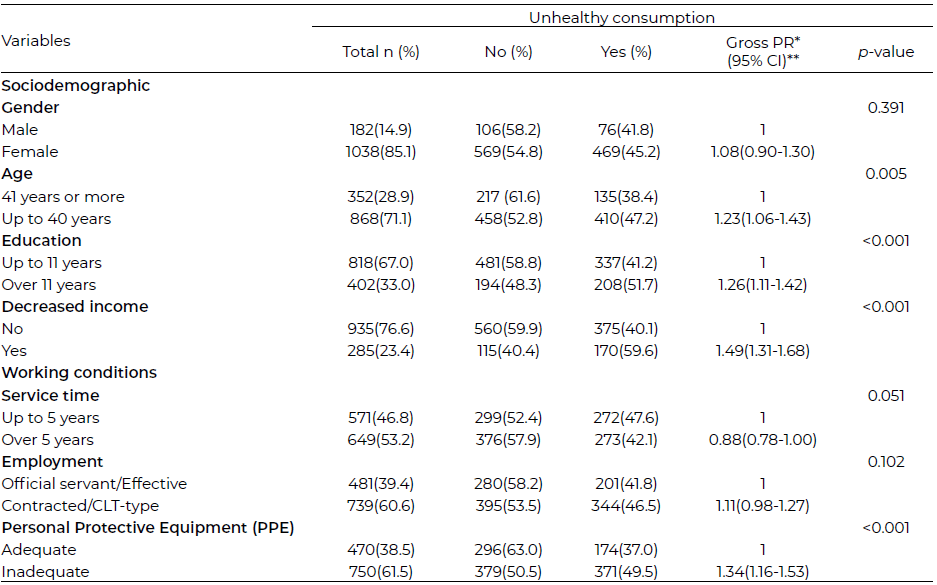
Note: * PR = Prevalence Ratio, ** CI = Confidence Interval
Table 2. Unhealthy food consumption among community health agents, according to health conditions and life habits in the north of Minas Gerais, 2020.
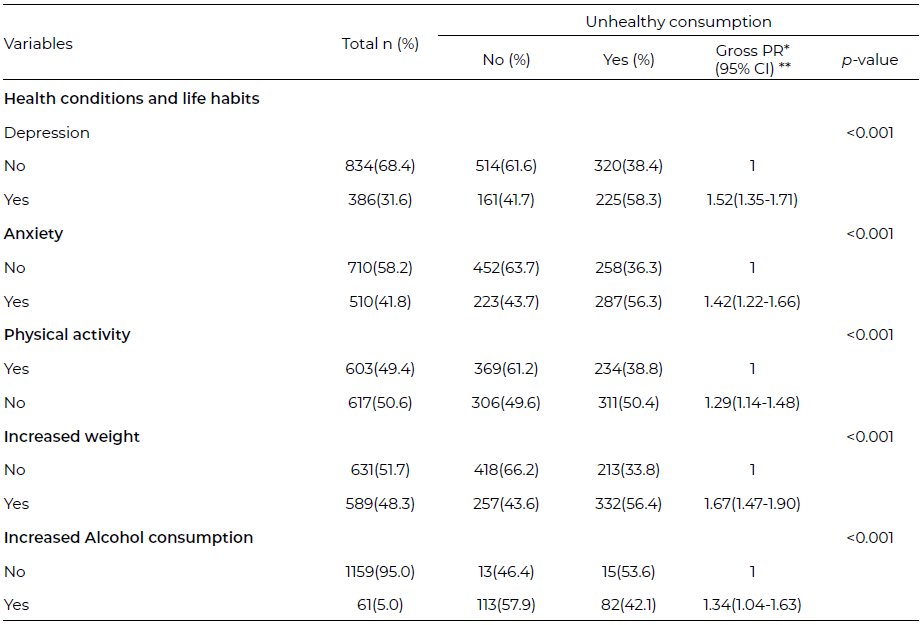
Note: * PR = Prevalence Ratio, ** CI = Confidence Interval
In this study, 44.7% of Community Health Workers (n = 545) reported unhealthy food consumption during the pandemic, Among CHWs, there was a 21.1% reduction in vegetable consumption and a 25.2% reduction in fruit consumption, while the consumption of sweets increased by 18.0% and the consumption of ultra-processed foods increased by 15.9%.
In the bivariate analysis between unhealthy consumption and the independent variables evaluated that showed significant association, level of 0.20, with the outcome were: age, education, decreased income, length of service, employment relationship, offer of EPIs, depression, anxiety, physical activity, weight gain and increased alcohol consumption.
The results of the multiple analysis are presented in Table 3. The Deviance test indicated that the model presented adequate fit quality (p-value =794.53). Unhealthy food consumption was more prevalent among community health agents aged 41 years or more (PR=1.34- 95%CI 1.05;1.71), schooling above 11 years of schooling (PR=1.17 - 95%CI 1.03;1.31), with decreased income (PR=1.35 - 95%CI 1.20;1.52) and inadequate offer of PPE (PR=1.20 - 95%CI 1.05-1.37).
Table 3. Poisson regression analysis, adjusted, of the variables associated with unhealthy food consumption among community health agents in the north of Minas Gerais, 2020.
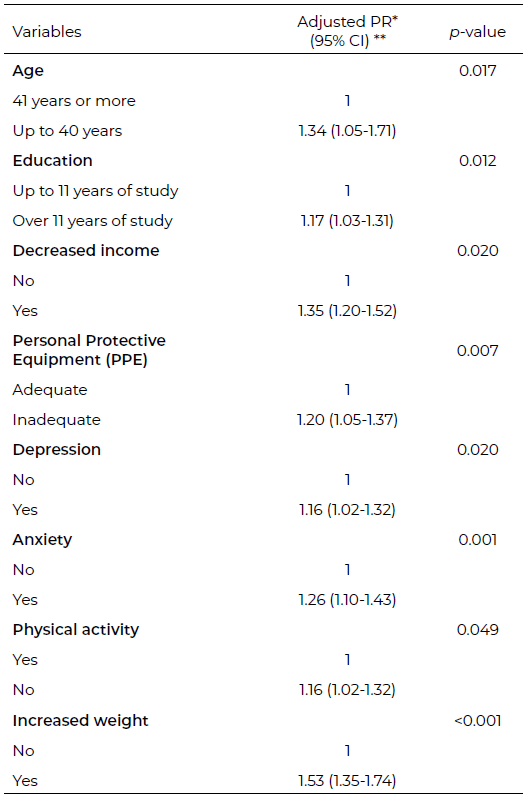
Note: * PR = Prevalence Ratio; ** CI = Confidence Interval; Omnibus 83.82 p-value= <0.001; Deviance=794.53; p-value = 0.656
As for health conditions and life habits, it was observed that the highest prevalence of unhealthy food consumption was among community health agents who have depression (PR=1.16 - 95%CI 1.02-1.32) and anxiety (PR=1.26 - 95%CI 1.10-1.43), non-practicing of physical activities (PR=1.16 - 95%CI 1.02-1.32) and weight gain (PR=1.53 - 95% CI 1.35-1.74).
Discussion
The findings of this study indicate a high prevalence of inadequate eating habits in CHW. A study conducted in Brazil in 2020 (13), presented how Brazilians reduced the consumption of healthy foods and increased that of ultra-processed and high energy density, such as chips, popcorn, chocolates and ice cream. In this sense, the increased intake of unhealthy foods results in health losses, such as increased obesity, hypertension, diabetes and cardiovascular diseases (14).
Although community health agents have knowledge about healthy lifestyle habits, the distance between knowledge and reported behavior is notorious (7). It is essential that health professionals assume healthy behaviors, so that they can influence their patients on the risk of chronic non-communicable diseases, and provide well-being among them (15).
It is also reiterated that the CHW has a role as a communicator between health and the population, being the holder of a community identity that reflects throughout the lifestyle of the community with which it relates. Thus, there is a need for a holistic valuation of these professionals, so that they can positively influence the quality of life of Brazilians (9).
Age up to 40 years was associated with food consumption. From this perspective, a study with data from the 2013 National Health Survey (PNS - Pesquisa Nacional de Saúde) regarding multidimensional profiles of lifestyle-related risk factors in adult individuals showed an association between lifestyles and sociodemographic characteristics. The healthy lifestyle was more present in older individuals, where several factors may be associated, such as greater awareness of health, greater concern due to the emergence of diseases and survival bias (16).
Of all the CHW who answered the questionnaire, 49.9% said they performed physical activity, and most of these had healthy food consumption. In contrast, a cross-sectional study that analyzed changes in the lifestyle of Brazilian adults showed that before the pandemic, 30.1% of people performed physical activity in contrast to only 12% during COVID-19 (13). The study confirms that compared to the general population, the number of CHW performing physical activity is higher and that unhealthy food consumption has a higher prevalence in the general population.
Weight gain was evidenced in 48.3% of the CHW. In the NutriNet coorte, the weight gain exceeded the weight loss (17). Weight gain can cause overweight or obesity and is associated with a higher prevalence of hypertension (18) and an increase in cardiovascular diseases (19).
Mental disorders are the cause of 9.5% of total disability-adjusted life years in Brazil, 35% of which are due to depressive disorders and 28% for anxiety disorders (20). Given their high prevalence and impact on functional capacity, examining circumstances that may influence mental health status in the present study population is particularly relevant. Symptoms of anxiety and depression are also prevalent among community health workers (CHWs) (21). Studies on the Psychiatry lifestyle have related some health behaviors, such as eating habits, to mental disorders, such as depression and anxiety (19). It was evident that the consumption of fruits and vegetables are associated with decreased risks and symptoms of depression (22). In addition, there was a strong association between the regular intake of soft drinks, sweets, ultra-processed foods and the substitution of lunch for quick snacks with the increased prevalence of depression (23).
The sociodemographic characteristics may influence the increase in overweight and obesity. In a previous study, higher prevalence rates of obesity were found in all age groups in females with less schooling (24). Study to investigate the variations of anthropometric indicators between 2013 and 2019 and the factors associated with obesity in Brazil, observed that for both males and females, factors associated with obesity were age, to live with a partner, level of instruction directly associated among men, and inversely associated among women (25).
The socioeconomic level and the educational level of individuals are associated with the lifestyle and, consequently, with obesity (24). This relationship is particularly relevant to the present study, as community health agents are both health workers and members of the communities they serve, and their living conditions may influence their own health behaviors. It is essential to implement intersectoral policies that expand access to healthy foods and promote the practice of physical activity, considering the economic, social, cultural, and environmental contexts of different population groups. For Community Health Workers, the adoption of healthy eating habits contributes to their own well-being and positively influences their professional performance. As health professionals who also serve as educators and role models within their communities, their practices can encourage healthier behaviors among the population, reinforcing the importance of supporting conditions that enable these habits (25).
A limitation of this study is the related to the data collection method. The use of an online questionnaire distributed via Google Forms and WhatsApp may have introduced selection bias, as participation depended on internet access, familiarity with digital tools, and voluntary engagement. Consequently, CHWs who were less connected to digital platforms or less available may be underrepresented in the sample. This should be considered when interpreting the findings.
The adoption of a healthy diet by the community health agents proved to be essential for the improvement of their well-being, in order to consequently impact positively on the exercise of the profession. Such eating habits, when placed under the parameter of the health professional, enable the provision of a better-quality service to the population, through this worker who acts not only as a caregiver, but also as an educator and model example.
Conclusions
The consumption of ultra-processed and high-energy-density foods was observed among Community Health Workers (CHWs) during the period evaluated. The factors associated with this dietary pattern, including age under 40 years, education level below 11 years, low income, limited or no availability of personal protective equipment (PPE), presence of depressive and anxiety symptoms, weight gain, and sedentary behavior. These findings reinforce the need for intervention strategies aimed at promoting healthier eating habits and lifestyle practices among CHWs. Such strategies may include nutrition education programs, psychosocial support actions, improved access to healthy foods within work environments, the creation of opportunities for regular physical activity, and the strengthening of occupational health policies. By addressing both individual and structural determinants, these interventions may contribute to improving the health and well-being of CHWs and enhancing their capacity to act as health promoters within the community.
Acknowledgments
We thank the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and the Universidade Estadual de Montes Claros (Unimontes) for the financial support.
Conflict of Interest
We declare that we have no conflict of interest, financial or affiliation.
References
- Brasil. Ministério da Saúde. Portaria nº 2.436, de 21 de setembro de 2017. Aprova a Política Nacional de Atenção Básica. Brasília, DF: Diário Oficial da União; 2017. https://bvsms.saude.gov.br/bvs/saudelegis/gm/2017/prt2436_22_09_2017.html
- Méllo LMB, Santos RC, Albuquerque PC. Community health workers: what do international studies tell us? Cien Saude Colet. 2023;28(2):501–520. https://doi.org/10.1590/1413-81232023282.12222022
- Dutra AFO, Dias ADC, Araujo DGS, Silva EM, Silva IMF, Gomes LMF. A importância da alimentação saudável e estado nutricional adequado frente a pandemia de Covid-19. Braz J Dev. 2020;6(9):66464-73. https://doi.org/10.34117/bjdv6n9-181
- Ferreira JN, Medeiros RLS, Bezerra YCP, Oliveira GS, Barros OQ. Community health workers: working conditions and occupational health. Rev Bras Med Trab. 2021;19(4):437–444. https://doi.org/10.47626/1679-4435-2021-622
- Nascimento VF, Terças ACP, Hattori TY, Graça BC, Cabral JF, Gleriano JS, et al. Dificuldades apontadas pelo agente comunitário de saúde na realização do seu trabalho. Saude. 2017;43(1):60-69. https://doi.org/10.5902/2236583423119
- Lima CCM, Fernandes TF, Pinho L, Rossi Barbosa LAR, Caldeira AP. O trabalho e os riscos de adoecimento dos agentes comunitários de saúde. Rev Psicol Organ Trab. 2024;24:e25225. https://doi.org/10.5935/rpot/2024.25225
- Oliveira RC, Figueiredo MF, Pereira ES, Granada GG. A pandemia de COVID-19 no Brasil favoreceu o consumo de alimentos ultraprocessados? Braz Appl Sci Rev. 2021;5(3):1297-1313. https://doi.org/10.34115/basrv5n3-002
- França CJ, Rocha PC, Pereira MLD, Silva GRF, Machado MH, Souza NVDO, et al. Características do trabalho do agente comunitário de saúde na pandemia de COVID-19 em municípios do Nordeste brasileiro. Cien Saude Colet. 2023;28(5):1399–1412. https://doi.org/10.1590/1413-81232023285.18422022
- Magalhães NP, Sousa PS, Pereira GV, Silveira MF, Brito MFSF, Rocha JSB, et al. Hábitos relacionados à saúde entre agentes comunitários de saúde de Montes Claros, Minas Gerais: estudo transversal, 2018. Epidemiol Serv Saude. 2021;30(3):e2020976. https://doi.org/10.1590/S1679-49742021000300002
- Fernandes TF, Lima CCM, Silva PLN, Rossi-Barbosa LAR, Pinho L, Caldeira AP. Condições de trabalho e saúde mental de agentes comunitários de saúde na pandemia de COVID-19. Cien Saude Colet. 2023;28(10):2931–2940. https://doi.org/10.1590/1413-812320232810.09802023
- Brasil. Ministério da Saúde. VIGITEL Brasil 2017: Vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Brasília: MS; 2018.
- Matsudo SM, Araújo T, Matsudo VR, Andrade D, Andrade E, Oliveira LC, et al. Questionário Internacional de Atividade Física (IPAQ): estudo de validade e reprodutibilidade no Brasil. Rev Bras Ativ Fis Saude. 2001;6(2):5-18. https://doi.org/10.12820/rbafs.v.6n2p5-18.
- Malta DC, Szwarcwald CL, Barros MB de A, Gomes CS, Machado ÍE, Souza Júnior PRB, et al. A pandemia da COVID-19 e as mudanças no estilo de vida dos brasileiros adultos: um estudo transversal, 2020. Epidemiol Serv Saude. 2020;29(4):e2020407. https://doi.org/10.1590/s1679-49742020000400026
- Pretto ADB, Pastore CA, Assunção MCF. Comportamentos relacionados à saúde entre profissionais de ambulatórios do Sistema Único de Saúde no município de Pelotas-RS. Epidemiol Serv Saude. 2014;23(4):635-644. https://doi.org/10.5123/S1679-49742014000400005
- Nunes MO, Trad LB, Almeida BA, Homem CR, Melo MCIC. O agente comunitário de saúde: construção da identidade desse personagem híbrido e polifônico. Cad Saude Publica. 2002;18(6):1639-1646. https://doi.org/10.1590/S0102-311X2002000600018
- Pereira IFS, Gonzaga MR, Lyra CO. Indicador multidimensional de fatores de risco relacionados ao estilo de vida: aplicação do método grade of membership. Cad Saude Publica. 2019; 35(6): e00124718. https://doi.org/10.1590/0102-311X00124718
- Costa CS, Steele EM, Leite MA, Rauber F, Levy RB, Monteiro CA. Mudanças de peso corporal na coorte NutriNet Brasil durante a pandemia de covid-19. Rev Saude Publica. 2021; 55:1. https://doi.org/10.11606/s1518-8787.2021055003457
- Donato TAA, Silva RMA, Andrade ACS, Kochergin CN, Medeiros DS, Soares DA, et al. Exame ocupacional periódico: oportunidade de diagnóstico e monitoramento de doença crônica não transmissível em homens. Cad Saude Publica. 2021;37:e00298320. https://doi.org/10.1590/0102-311X00298320
- Favarato D. Obesidade, gordura corporal e desfecho cardiovascular: além do índice de massa corporal. Arq Bras Cardiol. 2021;116(5):887-888. https://doi.org/10.36660/abc.20210074
- Souza MFM, França EB, Cavalcante A. Carga da doença e análise da situação de saúde: resultados da rede de trabalho do Global Burden of Disease (GBD) Brasil. Rev Bras Epidemiol. 2017;20(Suppl1):1-3. https://doi.org/10.1590/1980-5497201700050001
- Lima CCM, Fernandes TF, Barbosa MS, Rossi-Barbosa LAR, Pinho L, Caldeira AP. Análise dos indicadores de prazer e sofrimento no trabalho associados a ansiedade e depressão entre agentes comunitários de saúde. J Bras Psiquiatr. 2023;72(2):80–89. https://doi.org/10.1590/0047-208500000047
- Radavelli-Bagatini S, Anokye R, Bondonno NP, Sim M, Bondonno CP, Stanley MJ, et al. Association of habitual intake of fruits and vegetables with depressive symptoms: the AusDiab study. Eur J Nutr. 2021;60(7):3743-3755. https://doi.org/10.1007/s00394-021-02532-0
- Knüppel A, Shipley MJ, Llewellyn CH, Brunner EJ. Sugar intake from sweet food and beverages, common mental disorder and depression: prospective findings from the Whitehall II study. Sci Rep. 2017; 7:6287. https://doi.org/10.1038/s41598-017-05649-7
- Silva LES, Oliveira MM, Stopa SR, Gouvea ECDP, Ferreira KRD, Santos RO, et al. Tendência temporal da prevalência do excesso de peso e obesidade na população adulta brasileira, segundo características sociodemográficas, 2006-2019. Epidemiol Serv Saude. 2021;30(1):e2020294. https://doi.org/10.1590/S1679-49742021000100008
- Ferreira APS, Szwarcwald CL, Damacena GN, Souza Júnior PRB. Increasing trends in obesity prevalence from 2013 to 2019 and associated factors in Brazil. Rev Bras Epidemiol. 2021;24 (Suppl 2):e210009. https://doi.org/10.1590/1980-549720210009.supl.2
